Department of Surgery, University Hospital Monklands, Airdrie, Lanarkshire, UK.
Laparoscopic Biliary Service, University Hospital Monklands, Monkscourt Avenue, Airdrie, Lanarkshire, Scotland, ML6 0JS, UK.
Surg Endosc. 2022 Jan;36(1):550-558. doi: 10.1007/s00464-021-08316-1. Epub 2021 Feb 2.
Open conversion rates during laparoscopic cholecystectomy vary depending on many factors. Surgeon experience and operative difficulty influence the decision to convert on the grounds of patient safety but occasionally due to technical factors. We aim to evaluate the difficulties leading to conversion, the strategies used to minimise this event and how subspecialisation influenced conversion rates over time.
Prospectively collected data from 5738 laparoscopic cholecystectomies performed by a single surgeon over 28 years was analysed. Routine intraoperative cholangiography and common bile duct exploration when indicated are utilised. Patients undergoing conversion, fundus first dissection or subtotal cholecystectomy were identified and the causes and outcomes compared to those in the literature.
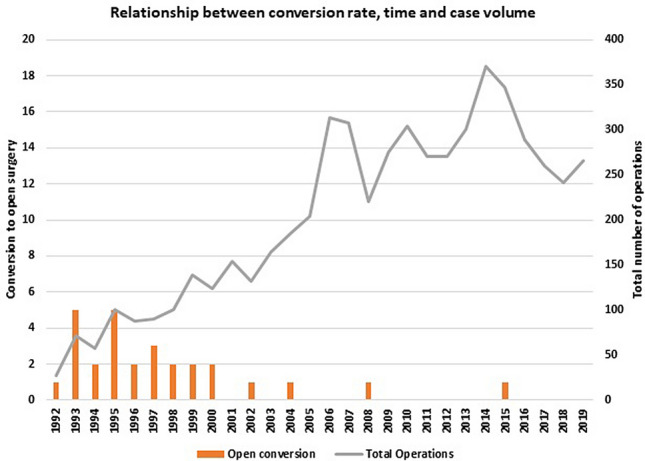
28 patients underwent conversion to open cholecystectomy (0.49%). Morbidity was relatively high (33%). 16 of the 28 patients (57%) had undergone bile duct exploration. The most common causes of conversion in our series were dense adhesions (9/28, 32%) and impacted bile duct stones (7/28, 25%). 173 patients underwent fundus first cholecystectomy (FFC) (3%) and 6 subtotal cholecystectomy (0.1%). Morbidity was 17.3% for the FFC and no complications were encountered in the subtotal cholecystectomy patients. These salvage techniques have reduced our conversion rate from a potential 3.5% to 0.49%.
Although open conversion should not be seen as a failure, it carries a high morbidity and should only be performed when other strategies have failed. Subspecialisation and a high emergency case volume together with FFC and subtotal cholecystectomy as salvage strategies can reduce conversion and its morbidity in difficult cholecystectomies.
腹腔镜胆囊切除术中转开腹的比率因多种因素而异。手术医生的经验和手术难度会影响基于患者安全的中转决策,但有时也会因为技术因素而中转。我们旨在评估导致中转的困难、用于将这种情况最小化的策略,以及亚专业领域如何随着时间的推移影响中转率。
对一名外科医生在 28 年期间进行的 5738 例腹腔镜胆囊切除术的前瞻性收集数据进行了分析。常规术中行胆管造影术,如果有必要,还会进行胆总管探查术。识别出中转、行胆囊底部先行解剖或行次全胆囊切除术的患者,并与文献中的结果进行比较。
28 例患者中转行开腹胆囊切除术(0.49%)。发病率相对较高(33%)。28 例患者中有 16 例行胆管探查术(57%)。在我们的系列中,最常见的中转原因是致密粘连(9/28,32%)和嵌顿性胆管结石(7/28,25%)。173 例行胆囊底部先行胆囊切除术(FFC)(3%),6 例行次全胆囊切除术(0.1%)。FFC 的发病率为 17.3%,次全胆囊切除术患者无并发症发生。这些抢救技术使我们的中转率从潜在的 3.5%降低到 0.49%。
虽然开放中转不应被视为失败,但它的发病率较高,只有在其他策略失败时才应进行。专业化和高急诊病例量,以及 FFC 和次全胆囊切除术作为抢救策略,可以降低困难性胆囊切除术中转及其发病率。