Sunnybrook Research Institute, Toronto, Ontario, Canada.
Department of Laboratory Medicine and Pathobiology, University of Toronto, Toronto, Ontario, Canada; and.
Am J Respir Crit Care Med. 2021 May 1;203(9):1112-1118. doi: 10.1164/rccm.202008-3070OC.
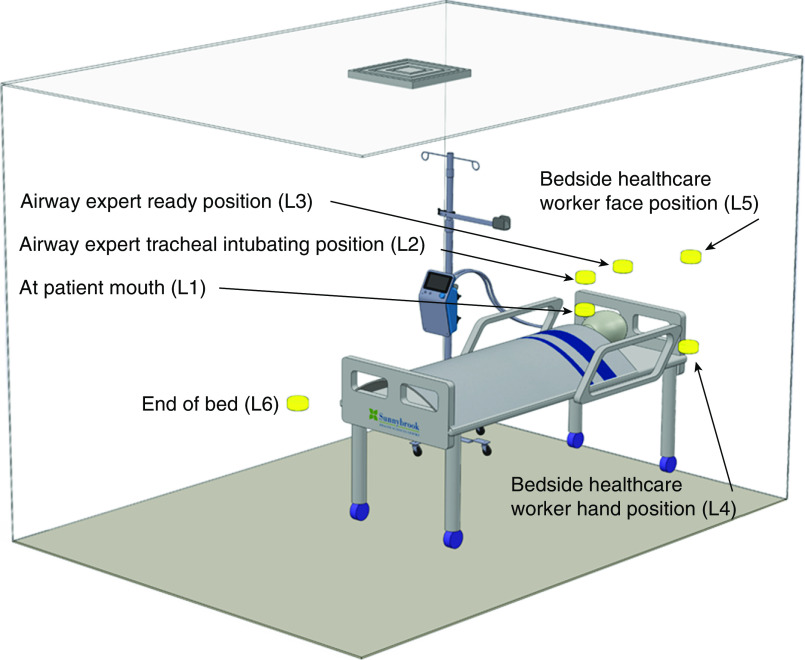
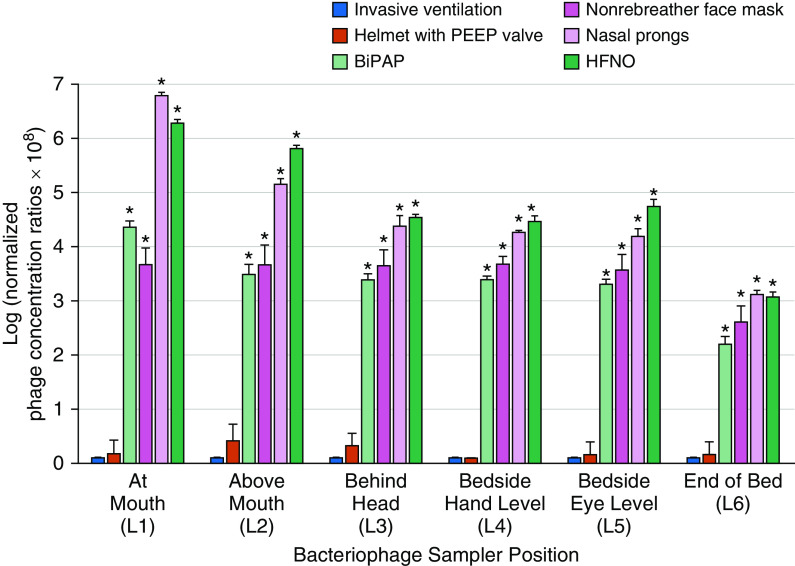
Patients with severe coronavirus disease (COVID-19) require supplemental oxygen and ventilatory support. It is unclear whether some respiratory support devices may increase the dispersion of infectious bioaerosols and thereby place healthcare workers at increased risk of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). To quantitatively compare viral dispersion from invasive and noninvasive respiratory support modalities. This study used a simulated ICU room with a breathing-patient simulator exhaling nebulized bacteriophages from the lower respiratory tract with various respiratory support modalities: invasive ventilation (through an endotracheal tube with an inflated cuff connected to a mechanical ventilator), helmet ventilation with a positive end-expiratory pressure (PEEP) valve, noninvasive bilevel positive-pressure ventilation, nonrebreather face masks, high-flow nasal oxygen (HFNO), and nasal prongs. Invasive ventilation and helmet ventilation with a PEEP valve were associated with the lowest bacteriophage concentrations in the air, and HFNO and nasal prongs were associated with the highest concentrations. At the intubating position, bacteriophage concentrations associated with HFNO (2.66 × 10 plaque-forming units [PFU]/L of air sampled), nasal prongs (1.60 × 10 PFU/L of air sampled), nonrebreather face masks (7.87 × 10 PFU/L of air sampled), and bilevel positive airway pressure (1.91 × 10 PFU/L of air sampled) were significantly higher than those associated with invasive ventilation ( < 0.05 for each). The difference between bacteriophage concentrations associated with helmet ventilation with a PEEP valve (4.29 × 10 PFU/L of air sampled) and bacteriophage concentrations associated with invasive ventilation was not statistically significant. These findings highlight the potential differential risk of dispersing virus among respiratory support devices and the importance of appropriate infection prevention and control practices and personal protective equipment for healthcare workers when caring for patients with transmissible respiratory viral infections such as SARS-CoV-2.
患有严重冠状病毒病 (COVID-19) 的患者需要补充氧气和通气支持。目前尚不清楚某些呼吸支持设备是否会增加传染性生物气溶胶的分散,从而使医护人员感染严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2) 的风险增加。为了定量比较来自侵入性和非侵入性呼吸支持方式的病毒分散。本研究使用模拟 ICU 房间,其中呼吸患者模拟器通过带膨胀袖口的气管内管从下呼吸道呼出雾化噬菌体,并使用各种呼吸支持方式:侵入性通气(通过带膨胀袖口的气管内管与机械通气机相连)、带呼气末正压 (PEEP) 阀的头盔通气、双水平正压通气、无重复呼吸面罩、高流量鼻氧 (HFNO) 和鼻插管。带 PEEP 阀的侵入性通气和头盔通气与空气中最低的噬菌体浓度相关,而 HFNO 和鼻插管与最高的浓度相关。在插管位置,与 HFNO(空气中采样的 2.66×10 噬菌斑形成单位 [PFU]/L)、鼻插管(空气中采样的 1.60×10 PFU/L)、无重复呼吸面罩(空气中采样的 7.87×10 PFU/L)和双水平正压气道(空气中采样的 1.91×10 PFU/L)相关的噬菌体浓度显着高于与侵入性通气相关的浓度(<0.05 每个)。带 PEEP 阀的头盔通气相关的噬菌体浓度(空气中采样的 4.29×10 PFU/L)与侵入性通气相关的噬菌体浓度之间的差异无统计学意义。这些发现强调了在呼吸支持设备中病毒分散的潜在差异风险,以及在照顾 SARS-CoV-2 等具有传染性呼吸道病毒感染的患者时,适当的感染预防和控制措施以及医护人员的个人防护设备的重要性。