Immunology Department, Beni-Messous Teaching Hospital, University of Algiers 1, Algeria.
Pneumology Department A, Béni-Messous Teaching Hospital, University of Algiers 1, Algeria.
Cytokine. 2021 May;141:155428. doi: 10.1016/j.cyto.2021.155428. Epub 2021 Jan 15.
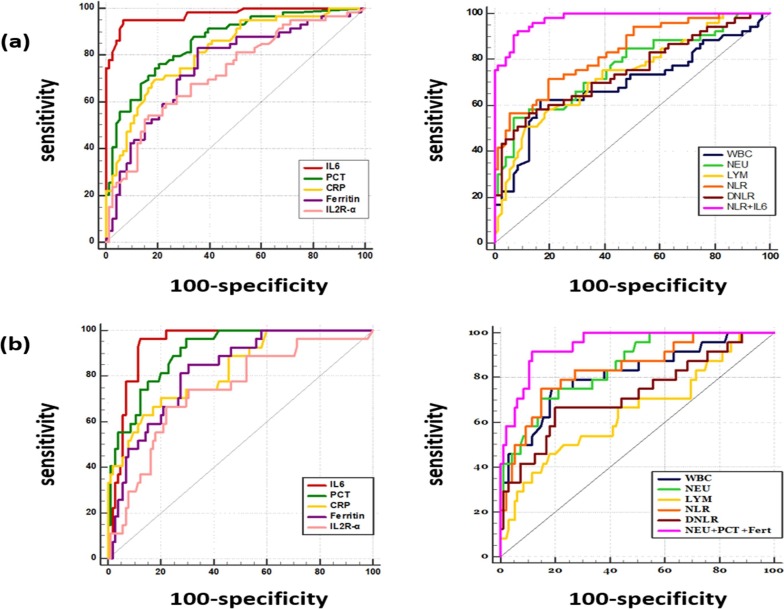
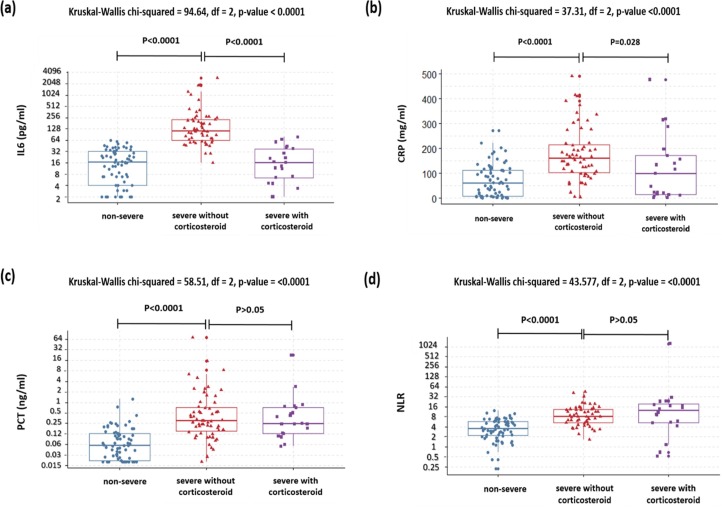
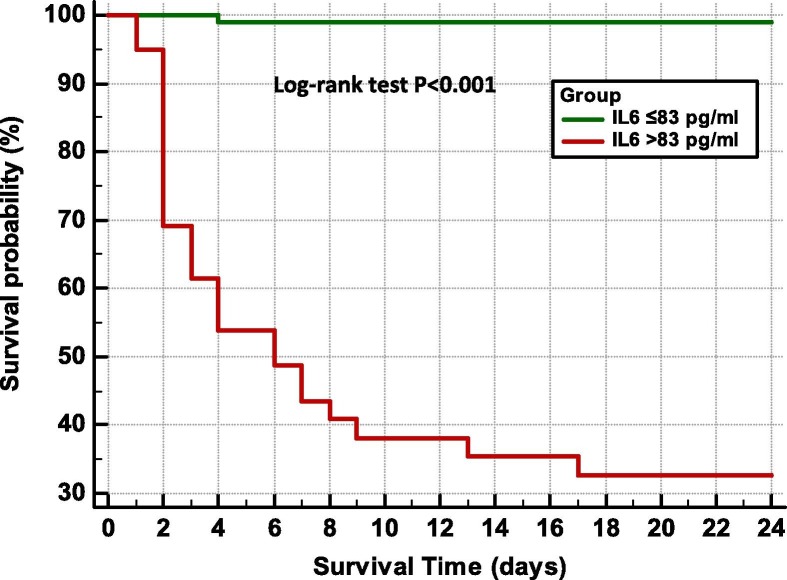
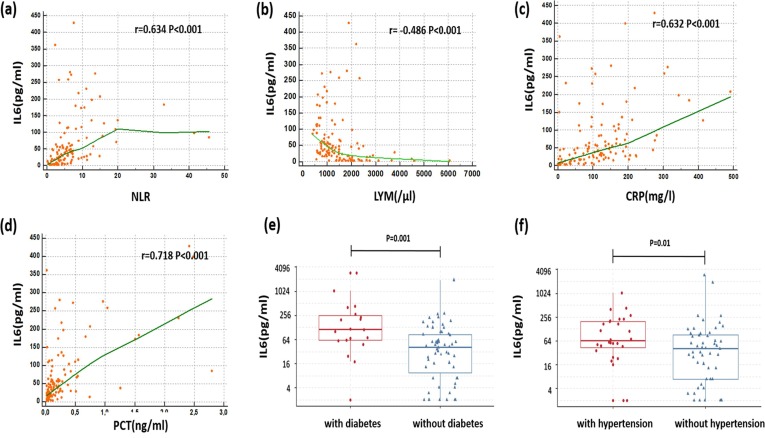
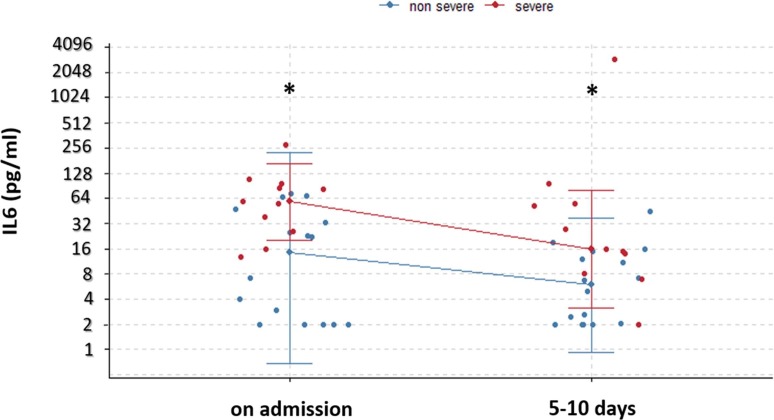
Accumulating evidence supports that the viral-induced hyper-inflammatory immune response plays a central role in COVID-19 pathogenesis. It might be involved in the progression to acute respiratory distress syndrome (ARDS), multi-organ failure leading to death. In this study, we aimed to evaluate the prognostic value of the immune-inflammatory biomarkers in COVID-19, then determine optimal thresholds for assessing severe and fatal forms of this disease.153 patients with confirmed COVID-19 were included in this study, and classified into non-severe and severe groups. Plasmatic levels of interleukin 6 (IL6), C-reactive protein (CRP), soluble-IL2 receptor (IL2Rα), procalcitonin (PCT) and ferritin were measured using chemiluminescence assay. Complete blood count was performed by Convergys 3X® hematology analyzer. Our results demonstrated that the peripheral blood levels of IL6, PCT, CRP, ferritin, IL2Rα, white blood cell count (WBC), neutrophil count (NEU), neutrophil-to-lymphocyte ratio (NLR), derived neutrophil-to-lymphocyte ratio (d-NLR) were significantly higher in severe forms of COVID-19. The ROC curve analysis showed that IL6 was the most accurate inflammatory biomarker. The calculated cutoff of IL6 (42 pg/ml) could correctly classify > 90% of patients regarding their risk of severity (area under ROC curve (AUROC) = 0.972) and the threshold value of 83 pg/ml was highly predictive of the progression to death (AUROC = 0.94, OR = 184) after a median of 3 days. Besides, IL-6 was positively correlated with other inflammatory markers and the kinetic analysis highlighted its value for monitoring COVID-19 patients. PCT and NLR had also a high prognostic relevance to assess severe forms of COVID-19 with corresponding AUROC of 0.856, 0.831 respectively. Furthermore the cut-off values of PCT (0.16 ng/ml) and NLR (7.4) allowed to predict mortality with high accuracy (se = 96.3%, sp = 70.5%,OR = 61.2)' (se = 75%, sp = 84%, OR = 14.6).The levels of these parameters were not influenced by corticosteroid treatment, which make them potential prognostic markers when patients are already undergoing steroid therapy.
越来越多的证据表明,病毒引起的过度炎症免疫反应在 COVID-19 的发病机制中起着核心作用。它可能与急性呼吸窘迫综合征(ARDS)的进展、多器官衰竭导致死亡有关。在这项研究中,我们旨在评估 COVID-19 中免疫炎症生物标志物的预后价值,然后确定评估这种疾病严重和致命形式的最佳阈值。
本研究纳入了 153 例确诊 COVID-19 的患者,并分为非重症组和重症组。采用化学发光法检测白细胞介素 6(IL6)、C 反应蛋白(CRP)、可溶性白细胞介素 2 受体(IL2Rα)、降钙素原(PCT)和铁蛋白的血浆水平。通过 Convergys 3X®血液分析仪进行全血细胞计数。
我们的结果表明,在 COVID-19 重症患者中,外周血白细胞介素 6(IL6)、PCT、CRP、铁蛋白、IL2Rα、白细胞计数(WBC)、中性粒细胞计数(NEU)、中性粒细胞与淋巴细胞比值(NLR)、衍生中性粒细胞与淋巴细胞比值(d-NLR)水平显著升高。ROC 曲线分析表明,IL6 是最准确的炎症生物标志物。计算得出的 IL6 截断值(42pg/ml)可以正确分类>90%的患者的严重风险(ROC 曲线下面积(AUROC)=0.972),而 83pg/ml 的阈值值高度预测中位时间为 3 天后死亡(AUROC=0.94,OR=184)。此外,IL-6 与其他炎症标志物呈正相关,其动力学分析突出了其监测 COVID-19 患者的价值。PCT 和 NLR 对评估 COVID-19 重症患者也具有较高的预后相关性,相应的 AUROC 分别为 0.856 和 0.831。此外,PCT(0.16ng/ml)和 NLR(7.4)的截断值可以高度准确地预测死亡率(se=96.3%,sp=70.5%,OR=61.2)(se=75%,sp=84%,OR=14.6)。这些参数的水平不受皮质类固醇治疗的影响,这使它们成为患者已经接受类固醇治疗时的潜在预后标志物。