Oak Ridge Institute for Science and Education, Oak Ridge, TN, USA.
Brandeis University, Waltham, MA, USA.
Inquiry. 2021 Jan-Dec;58:46958021991293. doi: 10.1177/0046958021991293.
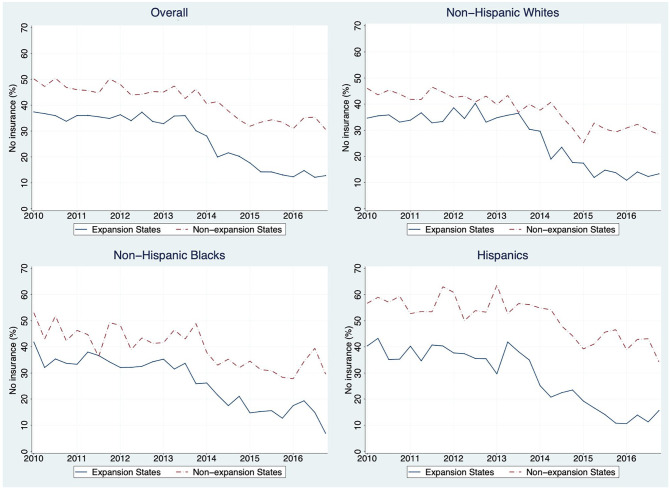
Since 2014, 32 states implemented Medicaid expansion by removing the categorical criteria for childless adults and by expanding income eligibility to 138% of the federal poverty level (FPL) for all non-elderly adults. Previous studies found that the Affordable Care Act (ACA) Medicaid expansion improved rates of being insured, unmet needs for care due to cost, number of physician visits, and health status among low-income adults. However, a few recent studies focused on the expansion's effect on racial/ethnic disparities and used the National Academy of Medicine (NAM) disparity approach with a limited set of access measures. This quasi-experimental study examined the effect of Medicaid expansion on racial/ethnic disparities in access to health care for U.S. citizens aged 19 to 64 with income below 138% of the federal poverty line. The difference-in-differences model compared changes over time in 2 measures of insurance coverage and 8 measures of access to health care, using National Health Interview Survey (NHIS) data from 2010 to 2016. Analyses used the NAM definition of disparities. Medicaid expansion was associated with significant decreases in uninsured rates and increases in Medicaid coverage among all racial/ethnic groups. There were differences across racial/ethnic groups regarding which specific access measures improved. For delayed care and unmet need for care, decreases in racial/ethnic disparities were observed. After the ACA Medicaid expansion, most access outcomes improved for disadvantaged groups, but also for others, with the result that disparities were not significantly reduced.
自 2014 年以来,32 个州通过取消对无子女成年人的分类标准,并将非老年成年人的收入资格扩大到联邦贫困线(FPL)的 138%,从而实施了医疗补助扩大计划。之前的研究发现,《平价医疗法案》(ACA)的医疗补助扩大计划提高了低收入成年人的保险覆盖率、因费用而无法获得医疗服务的比例、医生就诊次数和健康状况。然而,最近有一些研究集中在该计划对种族/族裔差异的影响上,并使用国家科学院医学研究所(NAM)的差异方法和一组有限的获得医疗服务的措施。这项准实验研究考察了医疗补助扩大计划对美国 19 至 64 岁、收入低于联邦贫困线 138%的公民获得医疗保健的种族/族裔差异的影响。差异中的差异模型比较了使用 2010 年至 2016 年全国健康访谈调查(NHIS)数据的 2 项保险覆盖措施和 8 项获得医疗保健措施的随时间变化。分析使用了 NAM 对差异的定义。医疗补助扩大计划与所有种族/族裔群体的未参保率下降和医疗补助覆盖率增加显著相关。在哪些特定的获得医疗服务的措施得到改善方面,不同种族/族裔群体存在差异。在延迟医疗服务和未满足的医疗服务需求方面,种族/族裔差异有所缩小。在 ACA 医疗补助扩大计划之后,大多数弱势群体和其他群体的获得医疗服务的结果都有所改善,因此差异没有显著减少。