Jestin Matthieu, Azoulay Elie, Pène Frédéric, Bruneel Fabrice, Mayaux Julien, Murgier Martin, Darmon Michael, Valade Sandrine
Service de Médecine Intensive Et Réanimation, Hôpital Saint-Louis, 1 Avenue Claude Vellefaux, 75010, Paris, France.
Université de Paris, 85 Boulevard Saint-Germain, 75006, Paris, France.
Ann Intensive Care. 2021 Feb 10;11(1):31. doi: 10.1186/s13613-021-00818-4.
Mucormycosis is an emerging fungal infection that may lead to multi-organ failure, especially in patients with hematological malignancies (HM). We performed a retrospective, cohort study, in five intensive care units (ICU) to assess the outcome of critically ill patients with HM and mucormycosis between 2002 and 2018. The secondary objective was to identify prognostic factors in this setting.
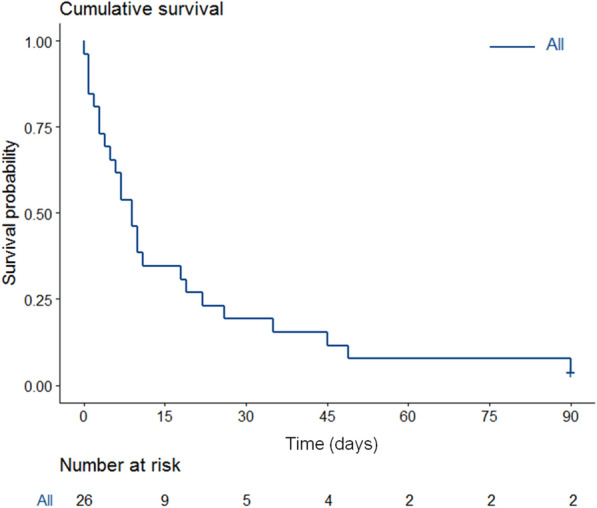
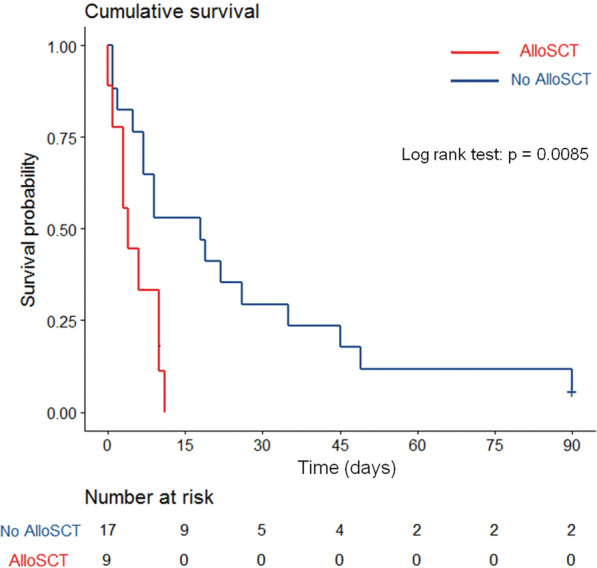
Twenty-six patients were included with a median age of 38 years [IQR, 26-57]). Acute leukemia was the most frequent underlying disease (50%). Nine patients (35%) underwent allogeneic stem cell transplantation (SCT). Nineteen patients (73%) had neutropenia and 16 (62%) had received steroids. The main reason for admission was acute respiratory failure (n = 14, 54%) followed by shock (n = 5 19%). The median SOFA score at admission was 7 [5-8]. According to EORTC/MSG criteria, mucormycosis was "proven" in 14 patients (54%), "probable" in 5 (19%) and "possible" in 7 (27%) in whom diagnosis was made by qPCR. Rhizopus and Mucor were the most frequent documented species. Seven patients (27%) had concurrent Aspergillus infection. Mucormycosis was diagnosed 1 day [-4 to + 6] after ICU admission. Sixteen patients (62%) had pulmonary involvement and ten (38%) rhino-cerebral involvement. Infection was disseminated in eight patients (31%). Twenty-two patients (85%) were treated with liposomal amphotericin B; 12 (46%) received antifungal combination including posaconazole in 7. Eight patients (31%) underwent curative surgery. Twenty-one patients (81%) required invasive mechanical ventilation (IMV), 18 (69%) vasopressors, and 9 (35%) renal replacement therapy. ICU and hospital mortality rates were 77% and 88%, respectively. The median overall survival was 9 days [3-22]. IMV was strongly associated with ICU mortality (p < 0.001) Three variables were associated with day 90 mortality in a Cox model including allogeneic SCT (HR 4.84 [95% CI 1.64-14.32]), SOFA score (1.19 [1.02-1.39]) and dual therapy (3.02 [1.18-7.72]).
Mucormycosis is associated with a high mortality rate in patients with HM, especially in allogeneic SCT recipients. Benefit of ICU management in these patients should be assessed before admission and strategies aiming to improve these patients' outcome are urgently needed.
毛霉病是一种新出现的真菌感染,可能导致多器官功能衰竭,尤其是在血液系统恶性肿瘤(HM)患者中。我们在五个重症监护病房(ICU)进行了一项回顾性队列研究,以评估2002年至2018年间患有HM和毛霉病的重症患者的预后。次要目标是确定这种情况下的预后因素。
纳入26例患者,中位年龄38岁[四分位间距,26 - 57岁])。急性白血病是最常见的基础疾病(50%)。9例患者(35%)接受了异基因干细胞移植(SCT)。19例患者(73%)有中性粒细胞减少症,16例(62%)接受过类固醇治疗。入院的主要原因是急性呼吸衰竭(n = 14,54%),其次是休克(n = 5,19%)。入院时的中位序贯器官衰竭评估(SOFA)评分是7[5 - 8]。根据欧洲癌症研究与治疗组织/侵袭性真菌感染协作组(EORTC/MSG)标准,14例患者(54%)的毛霉病为“确诊”,5例(19%)为“很可能”,7例(27%)为“可能”,后者通过定量聚合酶链反应(qPCR)确诊。根霉和毛霉是最常见的记录菌种。7例患者(27%)同时合并曲霉菌感染。毛霉病在ICU入院后1天[-4至 + 6]被诊断。16例患者(62%)有肺部受累,10例(38%)有鼻 - 脑受累。感染播散至8例患者(31%)。22例患者(85%)接受了脂质体两性霉素B治疗;12例(46%)接受了抗真菌联合治疗,其中7例包括泊沙康唑。8例患者(31%)接受了根治性手术。21例患者(81%)需要有创机械通气(IMV),18例(69%)需要血管活性药物,9例(35%)需要肾脏替代治疗。ICU死亡率和医院死亡率分别为77%和88%。中位总生存期为9天[3 - 22]。IMV与ICU死亡率密切相关(p < 0.001)。在一个Cox模型中,三个变量与90天死亡率相关,包括异基因SCT(风险比[HR] 4.84[95%置信区间(CI)1.64 - 14.32])、SOFA评分(1.19[1.02 - 1.39])和联合治疗(3.02[1.18 -