Academic Urology Unit, University of Sheffield, Sheffield, UK; Department of Urology, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK.
Leeds Institute of Medical Research at St James's and Leeds Institute for Data Analytics, University of Leeds, Leeds, UK.
Eur Urol. 2021 May;79(5):621-632. doi: 10.1016/j.eururo.2021.01.032. Epub 2021 Feb 10.
Little is known about health-related quality of life (HRQOL) following treatment for bladder cancer (BC).
To determine this, we undertook a cross-sectional survey covering 10% of the English population.
DESIGN, SETTING, AND PARTICIPANTS: Participants 1-10 yr from diagnosis were identified through national cancer registration data.
A postal survey was administered containing generic HRQOL and BC-specific outcome measures. Findings were compared with those of the general population and other pelvic cancer patients.
Generic HRQOL was measured using five-level EQ-5D (EQ-5D-5L) and European Organization for Research and Treatment of Cancer quality of life questionnaire (EORTC QLQ)-C30. BC-specific outcomes were derived from EORTC QLQ-BLM30 and EORTC QLQ-NMIBC24.
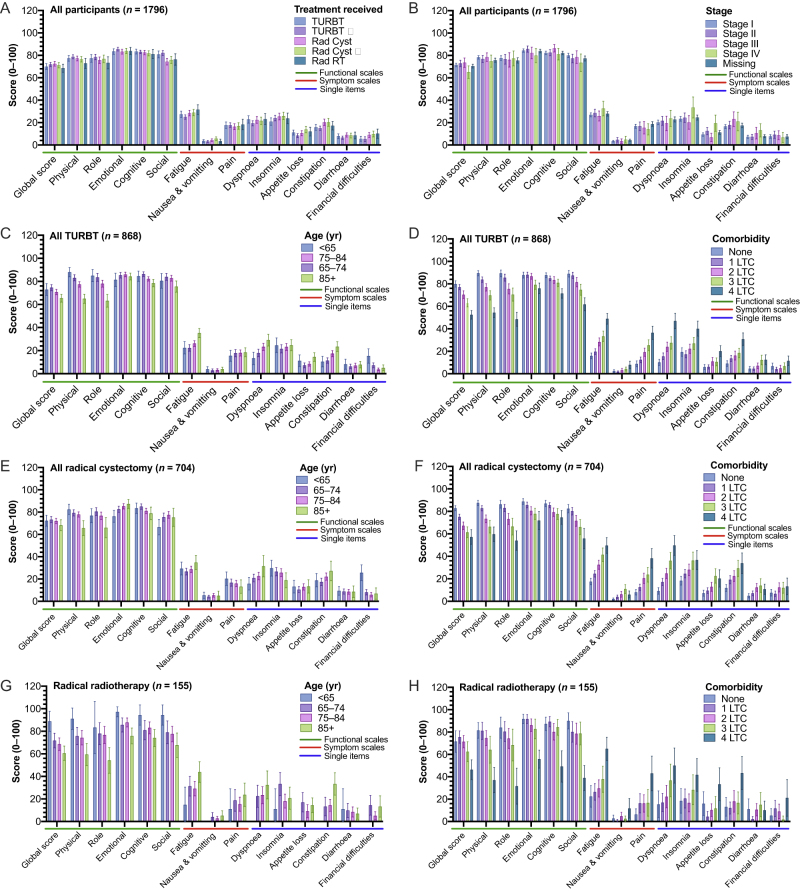
A total of 1796 surveys were completed (response rate 55%), including 868 (48%) patients with non-muscle-invasive BC, 893 (50%) patients who received radiotherapy or radical cystectomy, and 35 (1.9%) patients for whom treatment was unknown. Most (69%) of the participants reported at least one problem in any EQ-5D dimension. Age/sex-adjusted generic HRQOL outcomes were similar across all stages and treatment groups, whilst problems increased with age (problems in one or more EQ-5D dimensions: <65 yr [67% {95% confidence interval or CI: 61-74}] vs 85+ yr [84% {95% CI: 81-89}], p = 0.016) and long-term conditions (no conditions [53% {95% CI: 48-58}] vs more than four conditions [94% {95% CI: 90-97}], p < 0.001). Sexual problems were reported commonly in men, increasing with younger age and radical treatment. Younger participants (under 65 yr) reported more financial difficulties (mean score 20 [95% CI: 16-25]) than those aged 85+ yr (6.8 [4.5-9.2], p < 0.001). HRQOL for BC patients (for comparison, males with problems in one or more EQ-5D dimensions 69% [95% CI: 66-72]) was significantly worse than what has been found after colorectal and prostate cancers and in the general population (51% [95% CI: 48-53], all p < 0.05).
HRQOL following BC appears to be relatively independent of disease stage, treatment, and multimodal care. Issues are reported with sexual function and financial toxicity. HRQOL after BC is worse than that after other pelvic cancers.
Patients living with bladder cancer often have reduced quality of life, which may be worse than that for other common pelvic cancer patients. Age and other illnesses appear to be more important in determining this quality of life than the treatments received. Many men complain of sexual problems. Younger patients have financial worries.
膀胱癌(BC)治疗后,健康相关生活质量(HRQOL)的相关信息鲜为人知。
通过一项涵盖英国人口 10%的横断面调查来确定这一点。
设计、地点和参与者:通过国家癌症登记数据,确定了诊断后 1-10 年的参与者。
通过邮寄调查向参与者发放了通用 HRQOL 和 BC 特定的结果测量工具。将结果与一般人群和其他盆腔癌症患者进行了比较。
使用 5 级 EQ-5D(EQ-5D-5L)和欧洲癌症研究与治疗组织生活质量问卷(EORTC QLQ)-C30 测量通用 HRQOL。BC 特异性结果来自 EORTC QLQ-BLM30 和 EORTC QLQ-NMIBC24。
共完成了 1796 份调查问卷(应答率为 55%),其中包括 868 名非肌肉浸润性 BC 患者(48%)、893 名接受放疗或根治性膀胱切除术的患者(50%)和 35 名(1.9%)治疗未知的患者。大多数(69%)参与者在任何 EQ-5D 维度都报告了至少一个问题。在所有阶段和治疗组中,年龄/性别调整后的通用 HRQOL 结果相似,而随着年龄的增长问题会增加(在一个或多个 EQ-5D 维度中存在问题:<65 岁[61-74%] vs 85 岁以上[84-89%],p=0.016)和长期疾病(无疾病[53%] vs 四种以上疾病[94%],p<0.001)。男性经常报告性问题,随着年龄的降低和治疗方式的激进性,性问题也会增加。年轻的参与者(<65 岁)比 85 岁以上的参与者报告更多的经济困难(平均分数为 20 [95%CI:16-25])(p<0.001)。BC 患者的 HRQOL(相比之下,一个或多个 EQ-5D 维度存在问题的男性为 69%[95%CI:66-72%])明显差于结直肠癌和前列腺癌以及一般人群(51%[95%CI:48-53%],所有 p<0.05)。
BC 后的 HRQOL 似乎与疾病阶段、治疗和多模式护理相对独立。性功能和经济毒性方面存在问题。BC 后的 HRQOL 比其他盆腔癌症后更差。
患有膀胱癌的患者通常生活质量下降,这可能比其他常见的盆腔癌症患者更差。年龄和其他疾病似乎比所接受的治疗更能决定生活质量。许多男性抱怨性问题。年轻患者有经济上的担忧。