Department of Pediatric Hematology/Oncology, Cell and Gene Therapy, Scientific Institute for Research and Healthcare (IRCCS), Bambino Gesù Childrens' Hospital, Rome, Italy.
Sapienza, University of Rome, Rome, Italy.
Front Immunol. 2021 Jan 29;11:613644. doi: 10.3389/fimmu.2020.613644. eCollection 2020.
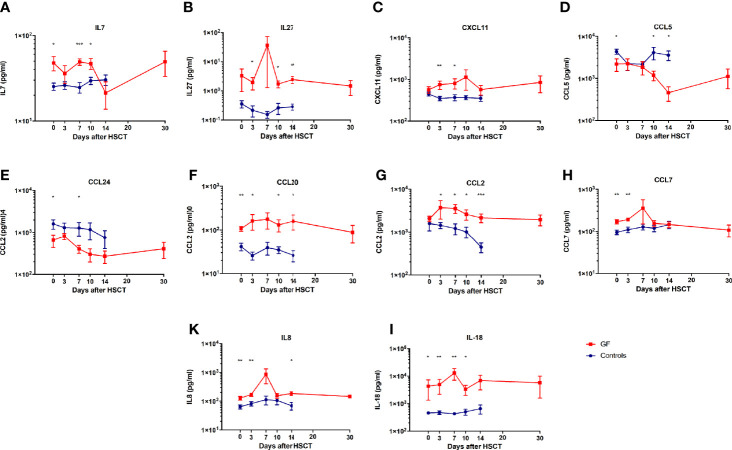
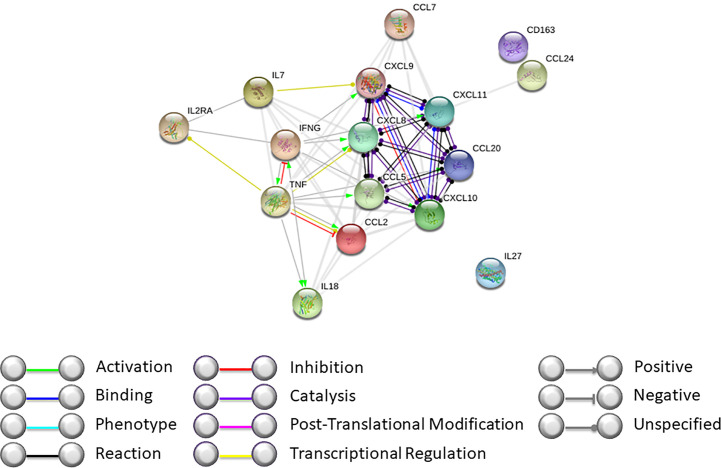
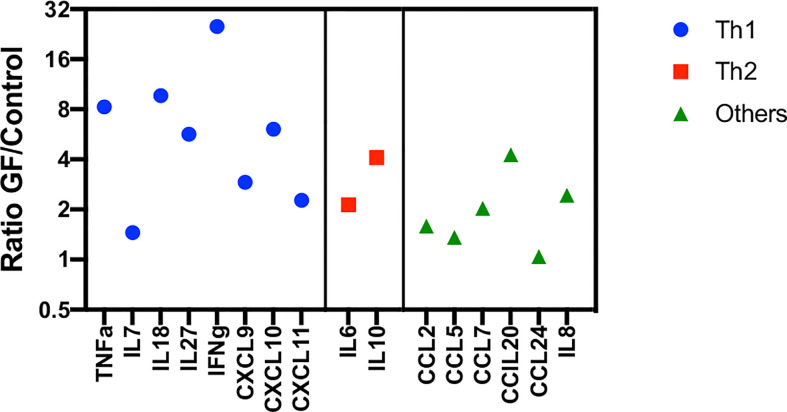
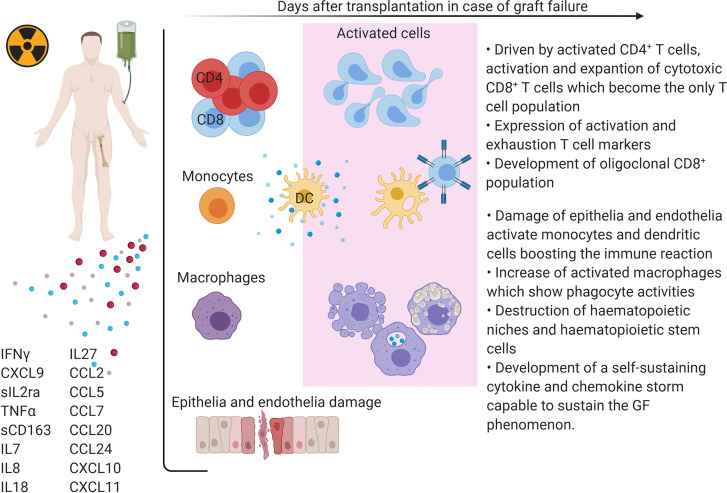
Graft failure is a severe complication of allogeneic hematopoietic stem cell transplantation (HSCT). The mechanisms involved in this phenomenon are still not completely understood; data available suggest that recipient T lymphocytes surviving the conditioning regimen are the main mediators of immune-mediated graft failure. So far, no predictive marker or early detection method is available. In order to identify a non-invasive and efficient strategy to diagnose this complication, as well as to find possible targets to prevent/treat it, we performed a detailed analysis of serum of eight patients experiencing graft failure after T-cell depleted HLA-haploidentical HSCT. In this study, we confirm data describing graft failure to be a complex phenomenon involving different components of the immune system, mainly driven by the IFNγ pathway. We observed a significant modulation of IL7, IL8, IL18, IL27, CCL2, CCL5 (Rantes), CCL7, CCL20 (MIP3a), CCL24 (Eotaxin2), and CXCL11 in patients experiencing graft failure, as compared to matched patients not developing this complication. For some of these factors, the difference was already present at the time of infusion of the graft, thus allowing early risk stratification. Moreover, these cytokines/chemokines could represent possible targets, providing the rationale for exploring new therapeutic/preventive strategies.
移植物失败是异基因造血干细胞移植(HSCT)的严重并发症。目前仍不完全了解涉及该现象的机制;现有数据表明,在预处理方案中存活下来的受者 T 淋巴细胞是免疫介导的移植物失败的主要介导者。到目前为止,还没有预测标志物或早期检测方法。为了确定一种非侵入性和有效的方法来诊断这种并发症,并找到可能的预防/治疗靶点,我们对 8 例接受 T 细胞耗竭 HLA 单倍体相合 HSCT 后发生移植物失败的患者的血清进行了详细分析。在这项研究中,我们证实了描述移植物失败是一种涉及免疫系统不同成分的复杂现象的数据,主要由 IFNγ 途径驱动。与未发生这种并发症的匹配患者相比,我们观察到发生移植物失败的患者中白细胞介素 7 (IL7)、白细胞介素 8 (IL8)、白细胞介素 18 (IL18)、白细胞介素 27 (IL27)、CC 趋化因子配体 2 (CCL2)、CC 趋化因子配体 5 (RANTES)、CCL7、CCL20 (MIP3a)、CCL24 (Eotaxin2)和 CXCL11 显著调节。对于其中一些因素,在输注移植物时就已经存在差异,从而允许早期风险分层。此外,这些细胞因子/趋化因子可能是潜在的治疗靶点,为探索新的治疗/预防策略提供了依据。