Division of Nephrology and Hypertension, Department of Internal Medicine, St Marianna University School of Medicine, Kawasaki.
Department of Nephrology, Kameda Medical Center, Chiba.
Medicine (Baltimore). 2021 Feb 5;100(5):e24460. doi: 10.1097/MD.0000000000024460.
Immunoglobulin A (IgA) nephropathy is a common heterogeneous kidney disease. One of the causes of secondary immunoglobulin A nephropathy is infection-related glomerulonephritis (IRGN), however, its accurate diagnosis is difficult.
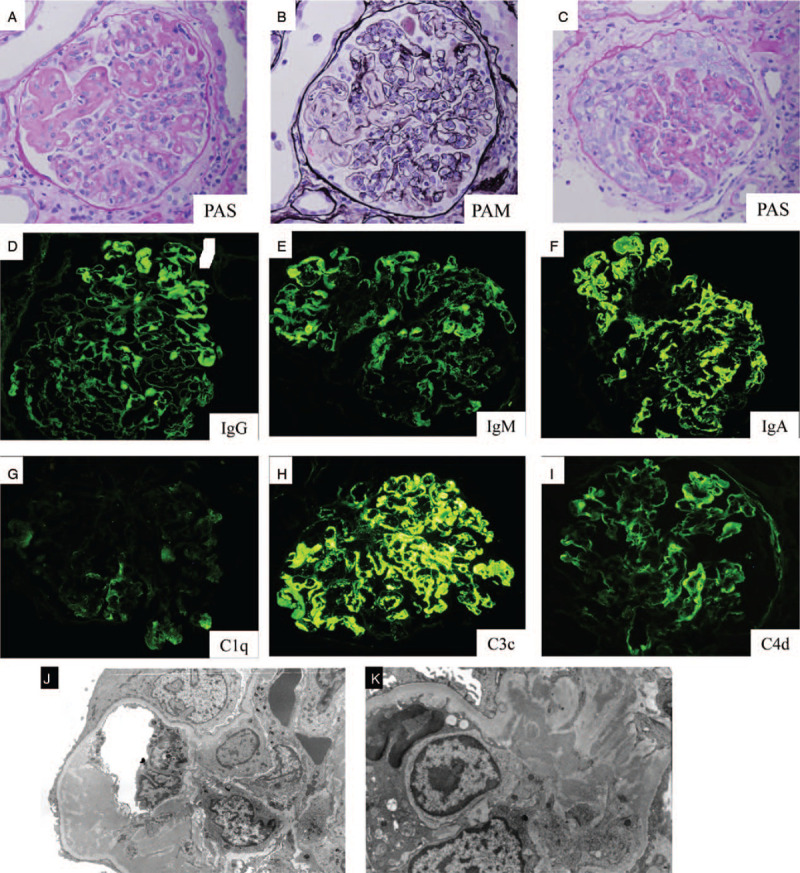
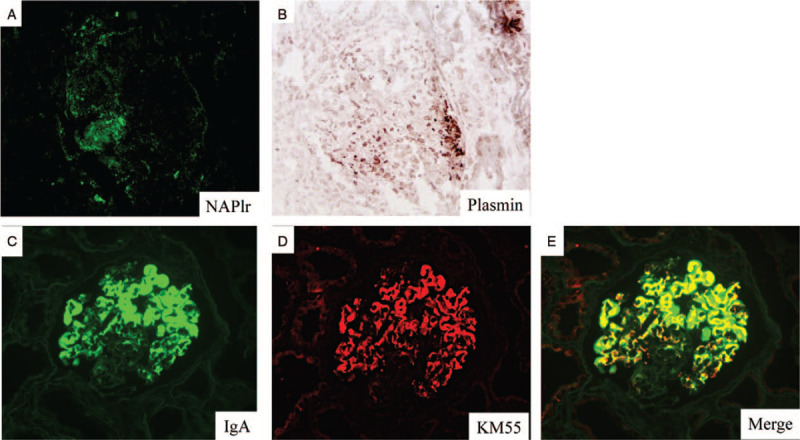
We report a rare case of an 82-year-old male presenting rapidly progressive glomerulonephritis. Assessment of a kidney biopsy by light microscopy revealed endocapillary glomerulonephritis with subendothelial deposits, such as wire loop lesions and cellular crescents. Immunofluorescence demonstrated strong staining for IgA and C3 along the glomerular capillary. Additional tests included positive staining for nephritis-associated plasmin receptor and positive plasmin activity in the glomeruli. Moreover, IgA and galactose-deficient IgA1 (Gd-IgA1) staining merged using immunofluorescence, followed by confirmation of high serum levels of Gd-IgA1 (9.3 μg/mL) by ELISA was observed.
The diagnosis of IgA-dominant IRGN was made.
We have initiated treatment with intravenous methylprednisolone 500 mg/day for 3 days, followed by oral prednisolone 25 mg/d as rapidly progressive glomerulonephritis. However immunosuppressive therapy was halted because of a poor response, and hemodialysis was initiated.
This is a case of IgA-dominant IRGN patient exhibiting positive glomerular staining for nephritis-associated plasmin receptor accompanied with high titers of serum Gd-IgA1. Our observations suggest that serum and kidney tissue of Gd-IgA1 may be useful for the diagnosis of IgA-dominant IRGN.
免疫球蛋白 A(IgA)肾病是一种常见的异质性肾脏疾病。继发性 IgA 肾病的一个病因是感染相关性肾小球肾炎(IRGN),然而,其准确诊断较为困难。
我们报告了一例罕见的 82 岁男性病例,其表现为快速进行性肾小球肾炎。肾脏活检的光镜评估显示内皮下肾小球肾炎伴内皮下沉积物,如线状病变和细胞性新月体。免疫荧光显示 IgA 和 C3 沿肾小球毛细血管呈强染色。其他检查包括肾炎相关纤溶酶受体阳性染色和肾小球内纤溶酶活性阳性。此外,免疫荧光观察到 IgA 和半乳糖缺乏 IgA1(Gd-IgA1)染色融合,随后通过 ELISA 观察到血清 Gd-IgA1 水平升高(9.3μg/ml)。
诊断为 IgA 主导的 IRGN。
我们开始使用静脉注射甲基强的松龙 500mg/天治疗 3 天,随后口服泼尼松 25mg/d 治疗快速进行性肾小球肾炎。然而,由于反应不佳,停止了免疫抑制治疗,并开始进行血液透析。
这是一例 IgA 主导的 IRGN 患者,其肾小球对肾炎相关纤溶酶受体呈阳性染色,同时伴有血清 Gd-IgA1 滴度升高。我们的观察结果表明,血清和肾脏组织中的 Gd-IgA1 可能有助于 IgA 主导的 IRGN 的诊断。