Zhang Chengcheng Christine, Liesenfeld Lukas, Klotz Rosa, Koschny Ronald, Rupp Christian, Schmidt Thomas, Diener Markus K, Müller-Stich Beat P, Hackert Thilo, Sauer Peter, Büchler Markus W, Schaible Anja
Department of Gastroenterology, Heidelberg University Hospital, University of Heidelberg, Im Neuenheimer Feld 410, 69120, Heidelberg, Germany.
Department of General, Visceral and Transplantation Surgery, Heidelberg University Hospital, Heidelberg, Germany.
BMC Gastroenterol. 2021 Feb 16;21(1):72. doi: 10.1186/s12876-021-01651-6.
Anastomotic leakage (AL) in the upper gastrointestinal (GI) tract is associated with high morbidity and mortality rates. Especially intrathoracic anastomotic leakage leads to life-threatening complications. Endoscopic vacuum therapy (EVT) for anastomotic leakage after transthoracic esophageal resection represents a novel concept. However, sound clinical data are still scarce. This retrospective, single-center study aimed to evaluate the feasibility, effectiveness, and safety of EVT for intrathoracic anastomotic leakage following abdomino-thoracic esophageal resection.
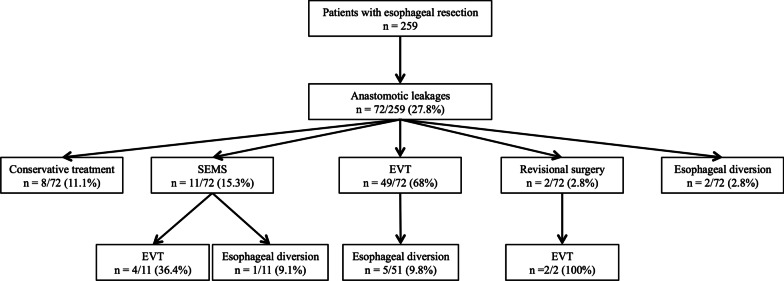
From March 2014 to September 2019 259 consecutive patients underwent elective transthoracic esophageal resection. 72 patients (27.8%) suffered from AL. The overall collective in-hospital mortality rate was 3.9% (n = 10). Data from those who underwent treatment with EVT were included.
Fifty-five patients were treated with EVT. Successful closure was achieved in 89.1% (n = 49) by EVT only. The EVT-associated complication rate was 5.4% (n = 3): bleeding occurred in one patient, while minor sedation-related complications were observed in two patients. The median number of EVT procedures per patient was 3. The procedures were performed at intervals of 3-5 days, with a 14-day median duration of therapy. The mortality rate of patients with AL was 7.2% (n = 4). Despite successfully terminated EVT, three patients died because of multiple organ failure, acute respiratory distress syndrome, and urosepsis (5.4%). One patient (1.8%) died during EVT due to cardiac arrest.
EVT is a safe and effective approach for intrathoracic anastomotic leakages following abdomino-thoracic esophageal resections. It offers a high leakage-closure rate and the potential to lower leakage-related mortalities.
This trial was registered and approved by the Institutional Ethics Committee of the University of Heidelberg on 16.04.2014 (Registration Number: S-635/2013).
上消化道吻合口漏与高发病率和死亡率相关。尤其是胸内吻合口漏会导致危及生命的并发症。经胸段食管切除术后吻合口漏的内镜下真空治疗是一种新概念。然而,可靠的临床数据仍然匮乏。这项回顾性单中心研究旨在评估经胸段食管切除术后内镜下真空治疗对胸内吻合口漏的可行性、有效性和安全性。
2014年3月至2019年9月,259例连续患者接受了择期经胸段食管切除术。72例患者(27.8%)发生了吻合口漏。总体住院死亡率为3.9%(n = 10)。纳入接受内镜下真空治疗患者的数据。
55例患者接受了内镜下真空治疗。仅通过内镜下真空治疗,89.1%(n = 49)实现了成功闭合。内镜下真空治疗相关并发症发生率为5.4%(n = 3):1例患者发生出血,2例患者出现轻微的镇静相关并发症。每位患者内镜下真空治疗的中位数为3次。治疗间隔为3至5天,中位治疗持续时间为14天。吻合口漏患者的死亡率为7.2%(n = 4)。尽管内镜下真空治疗成功结束,但3例患者因多器官功能衰竭、急性呼吸窘迫综合征和尿脓毒症死亡(5.4%)。1例患者(1.8%)在内镜下真空治疗期间因心脏骤停死亡。
内镜下真空治疗是经胸段食管切除术后胸内吻合口漏的一种安全有效的方法。它具有较高的漏口闭合率和降低漏口相关死亡率的潜力。
本试验于2014年4月16日由海德堡大学机构伦理委员会注册并批准(注册号:S-635/2013)。