Royal Free London NHS Foundation Trust, Pond Street, London NW3 2QG, UK.
Institute of Cardiovascular Science, University College London, UK.
Eur Heart J. 2021 May 14;42(19):1866-1878. doi: 10.1093/eurheartj/ehab075.
Troponin elevation is common in hospitalized COVID-19 patients, but underlying aetiologies are ill-defined. We used multi-parametric cardiovascular magnetic resonance (CMR) to assess myocardial injury in recovered COVID-19 patients.
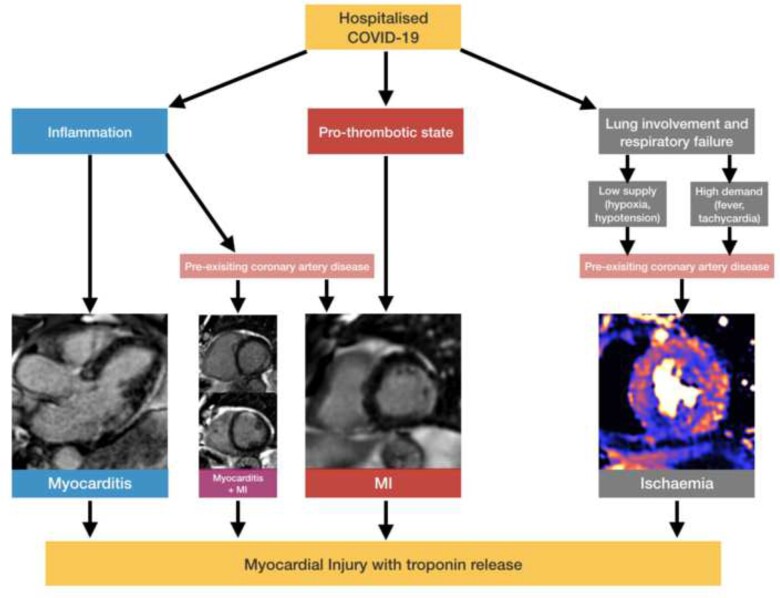
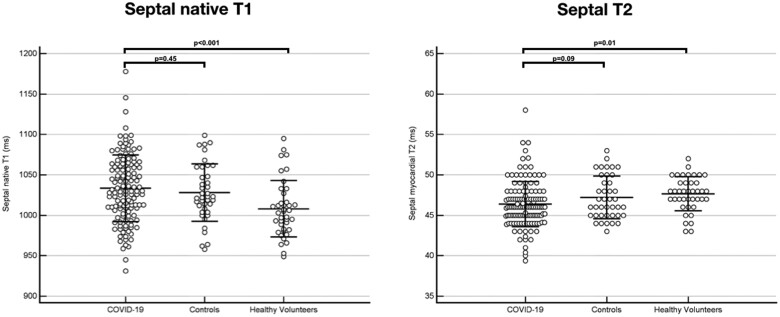
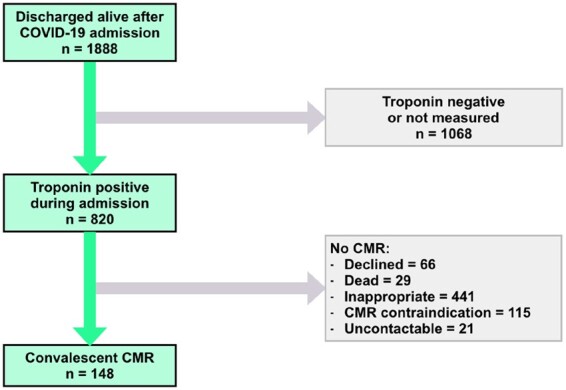
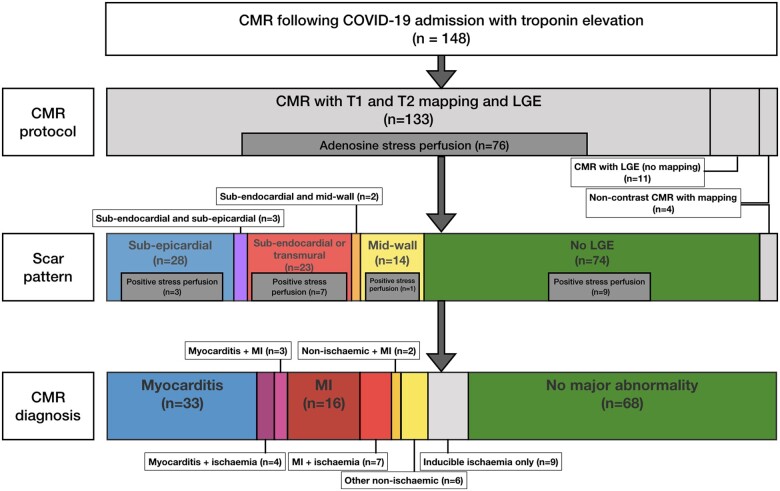
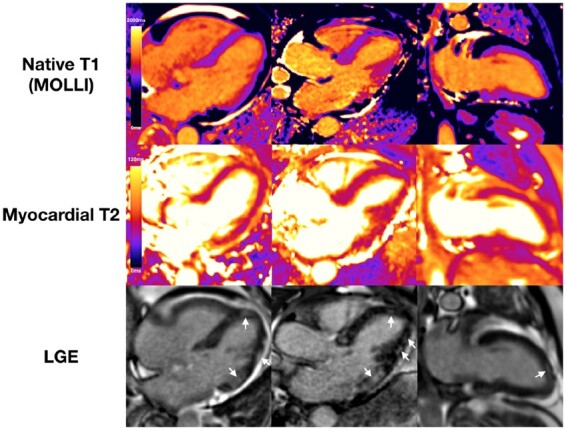
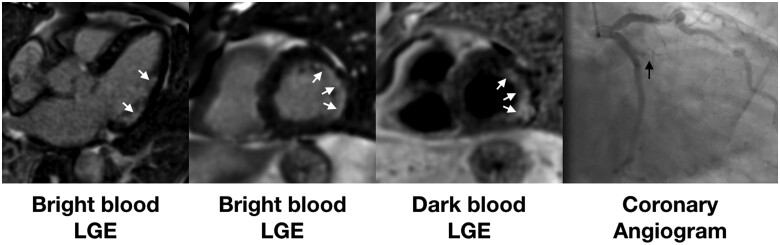
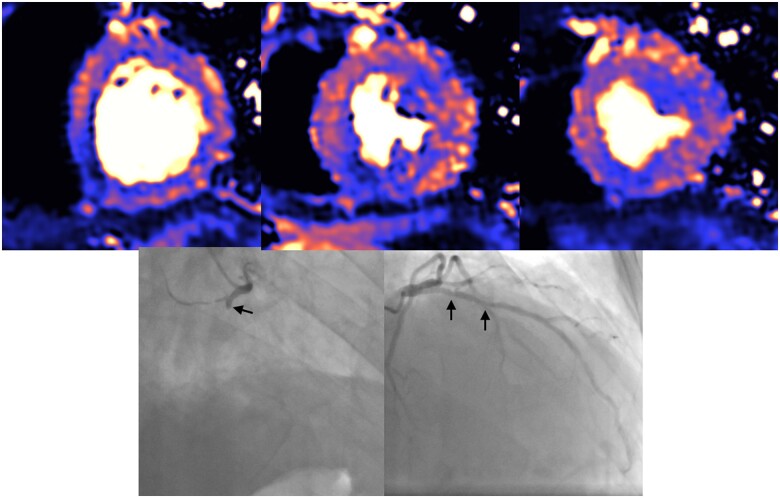
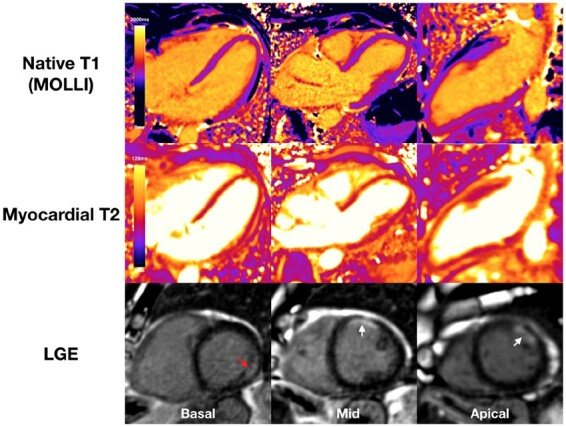
One hundred and forty-eight patients (64 ± 12 years, 70% male) with severe COVID-19 infection [all requiring hospital admission, 48 (32%) requiring ventilatory support] and troponin elevation discharged from six hospitals underwent convalescent CMR (including adenosine stress perfusion if indicated) at median 68 days. Left ventricular (LV) function was normal in 89% (ejection fraction 67% ± 11%). Late gadolinium enhancement and/or ischaemia was found in 54% (80/148). This comprised myocarditis-like scar in 26% (39/148), infarction and/or ischaemia in 22% (32/148) and dual pathology in 6% (9/148). Myocarditis-like injury was limited to three or less myocardial segments in 88% (35/40) of cases with no associated LV dysfunction; of these, 30% had active myocarditis. Myocardial infarction was found in 19% (28/148) and inducible ischaemia in 26% (20/76) of those undergoing stress perfusion (including 7 with both infarction and ischaemia). Of patients with ischaemic injury pattern, 66% (27/41) had no past history of coronary disease. There was no evidence of diffuse fibrosis or oedema in the remote myocardium (T1: COVID-19 patients 1033 ± 41 ms vs. matched controls 1028 ± 35 ms; T2: COVID-19 46 ± 3 ms vs. matched controls 47 ± 3 ms).
During convalescence after severe COVID-19 infection with troponin elevation, myocarditis-like injury can be encountered, with limited extent and minimal functional consequence. In a proportion of patients, there is evidence of possible ongoing localized inflammation. A quarter of patients had ischaemic heart disease, of which two-thirds had no previous history. Whether these observed findings represent pre-existing clinically silent disease or de novo COVID-19-related changes remain undetermined. Diffuse oedema or fibrosis was not detected.
肌钙蛋白升高在住院的 COVID-19 患者中很常见,但潜在的病因尚不清楚。我们使用多参数心血管磁共振(CMR)评估康复的 COVID-19 患者的心肌损伤。
148 名患有严重 COVID-19 感染的患者(64±12 岁,70%为男性)[均需要住院治疗,48%(32%)需要通气支持]在六家医院接受了恢复期 CMR(如果有指征则包括腺苷应激灌注),中位数为 68 天。89%(射血分数 67%±11%)的左心室(LV)功能正常。54%(80/148)发现晚期钆增强和/或缺血。这包括心肌炎样瘢痕 26%(39/148)、梗死和/或缺血 22%(32/148)和双重病理学 6%(9/148)。心肌炎样损伤在 88%(35/40)的病例中局限于三个或更少的心肌节段,且无相关 LV 功能障碍;其中 30%有活动性心肌炎。在接受应激灌注的患者中发现心肌梗死 19%(28/148)和可诱导缺血 26%(20/76)(包括 7 例既有梗死又有缺血)。有缺血性损伤模式的患者中,66%(27/41)无既往冠心病史。在远程心肌中没有弥漫性纤维化或水肿的证据(T1:COVID-19 患者 1033±41 ms 与匹配对照 1028±35 ms;T2:COVID-19 46±3 ms 与匹配对照 47±3 ms)。
在 COVID-19 严重感染后伴有肌钙蛋白升高的恢复期,可能会出现心肌炎样损伤,其范围有限,功能后果极小。在一部分患者中,有证据表明可能存在持续的局部炎症。四分之一的患者有缺血性心脏病,其中三分之二无既往病史。这些观察到的发现是代表先前存在的临床无症状疾病还是新出现的 COVID-19 相关变化仍未确定。未发现弥漫性水肿或纤维化。