Mazza Manuela
Department of Anaesthesiology, Critical Care Medicine and Pain Medicine, Nuovo Ospedale degli Infermi, Via dei Ponderanesi 2, Biella, Ponderano, Italy.
J Cannabis Res. 2021 Feb 17;3(1):4. doi: 10.1186/s42238-021-00060-6.
The use of cannabis for treating fibromyalgia syndrome (FMS) has not been comprehensively investigated. Thus, we have assessed the efficacy and adverse events (AEs) of short- and long-term medical cannabis (MC) treatment for FMS.
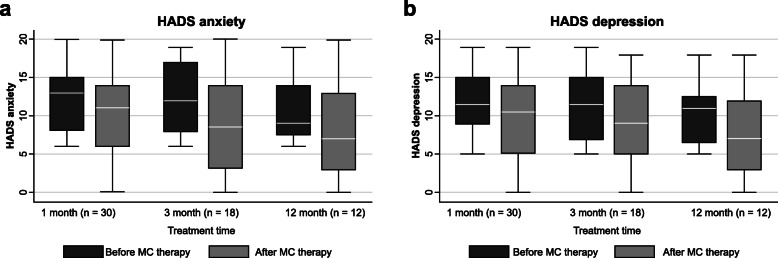
Data were obtained from medical reports archived in the pain clinic of Ponderano (Italy; retrospective study). FMS patients, who were resistant to conventional therapy, received licensed MC with various Δ-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) content, as powdered whole flowers (decoction or vaporization) or oil extracts. Demographic and clinical parameters, including Numerical Rating Scale (NRS), Oswestry Disability Index (ODI), Hospital Anxiety and Depression Scale, Widespread Pain Index (WPI), Severity Score (SyS), and side effects, were obtained after 1, 3, and 12 months. Data were analyzed with Wilcoxon signed-rank tests for paired data.
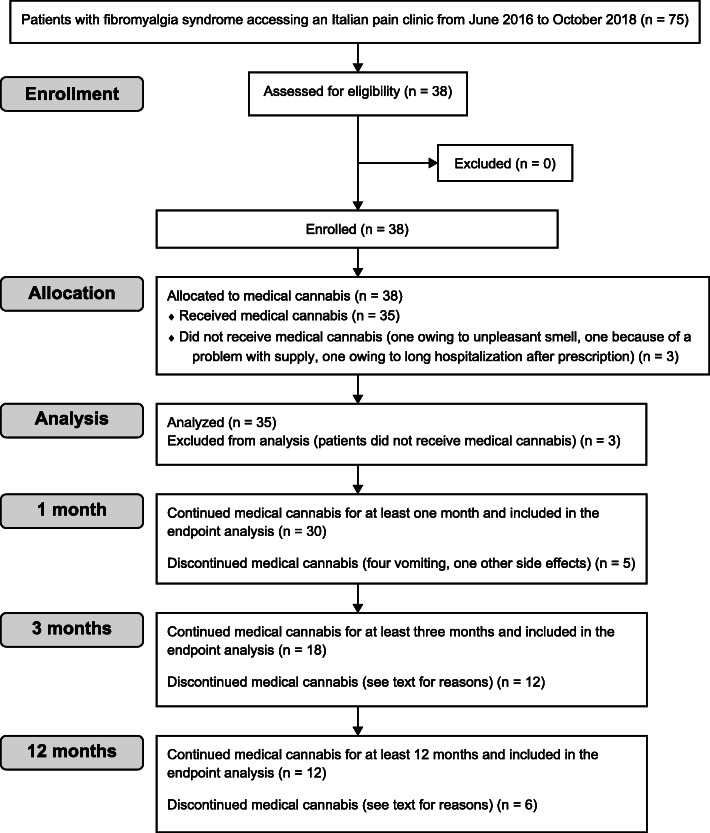
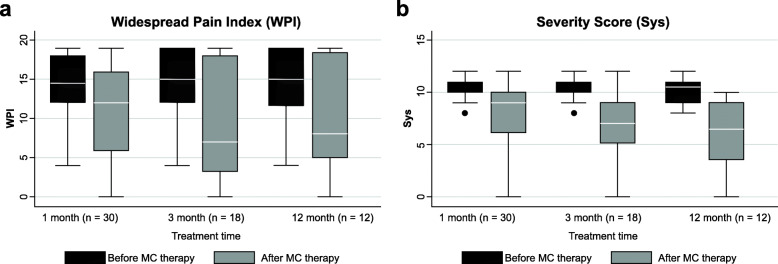
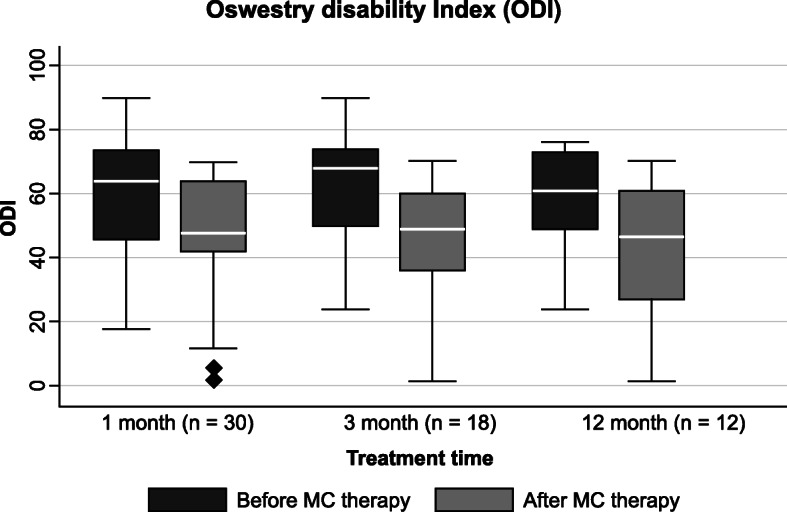
Thirty-eight patients were included. Thirty, 18, and 12 patients continued therapy for 1, 3, and 12 months, respectively. Significant improvements (p < 0.01) were observed in NRS, ODI, WPI, and SyS at 1 month; in NRS, ODI, and WPI at 3 months; and in NRS, ODI, and SyS at 12 months. Therapy was interrupted by 17 patients (48.6%) owing to nonserious AEs according to the FDA. The most common side effects were mental confusion (37%), dizziness (14%), nausea/vomiting (14%), and restlessness/irritation (14%). The median daily dose of milled flowers administered as THC-dominant MC and hybrid MC (with similar THC/CBD ratio) was 200 mg/day and 400 mg/day, respectively. After 3 months of titration, the median content of THC administered with THC-dominant MC cultivars was 46.2 mg, and of THC + CBD administered as a hybrid MC cultivar, was 23.6 mg + 38 mg. At 3 months, median THC content administered in the oil extract of the THC-dominant MC cultivars was 9.7 mg, while that of THC + CBD administered in the oil extract of the hybrid MC cultivars was 1.8 mg + 2 mg.
MC may represent an alternative treatment for patients with FMS who are unresponsive to conventional therapy. However, its application may be limited by the incidence of nonserious AEs.
大麻用于治疗纤维肌痛综合征(FMS)尚未得到全面研究。因此,我们评估了短期和长期医用大麻(MC)治疗FMS的疗效和不良事件(AE)。
数据来自意大利庞德拉诺疼痛诊所存档的医疗报告(回顾性研究)。对传统治疗耐药的FMS患者接受了含不同Δ-9-四氢大麻酚(THC)和大麻二酚(CBD)含量的合法MC,形式为全花粉末(煎剂或汽化剂)或油提取物。在1、3和12个月后获取人口统计学和临床参数,包括数字评定量表(NRS)、奥斯威斯残疾指数(ODI)、医院焦虑抑郁量表、广泛性疼痛指数(WPI)、严重程度评分(SyS)以及副作用。对配对数据采用Wilcoxon符号秩检验进行数据分析。
纳入38例患者。分别有30、18和12例患者持续治疗1、3和12个月。在1个月时,NRS、ODI、WPI和SyS有显著改善(p<0.01);3个月时,NRS、ODI和WPI有显著改善;12个月时,NRS、ODI和SyS有显著改善。17例患者(48.6%)因美国食品药品监督管理局(FDA)认定的非严重AE中断治疗。最常见的副作用是精神错乱(37%)、头晕(14%)、恶心/呕吐(14%)和烦躁不安/易怒(14%)。以THC为主的MC和混合MC(THC/CBD比例相似)形式给药的碾碎花朵的每日中位剂量分别为200毫克/天和400毫克/天。经过3个月的滴定,以THC为主的MC品种给药的THC中位含量为46.2毫克,以混合MC品种给药的THC + CBD中位含量为23.6毫克 + 38毫克。在3个月时,以THC为主的MC品种油提取物中给药的THC中位含量为9.7毫克,而混合MC品种油提取物中给药的THC + CBD中位含量为1.8毫克 + 2毫克。
MC可能是对传统治疗无反应的FMS患者的一种替代治疗方法。然而,其应用可能受到非严重AE发生率的限制。