Department of Oncology, University of Oxford, Oxford, England, United Kingdom.
Department of Oncology, Oxford University Hospitals National Health Service Foundation Trust, Oxford, England, United Kingdom.
Clin Cancer Res. 2021 May 1;27(9):2459-2469. doi: 10.1158/1078-0432.CCR-20-4128. Epub 2021 Feb 17.
Tumor hypoxia fuels an aggressive tumor phenotype and confers resistance to anticancer treatments. We conducted a clinical trial to determine whether the antimalarial drug atovaquone, a known mitochondrial inhibitor, reduces hypoxia in non-small cell lung cancer (NSCLC).
Patients with NSCLC scheduled for surgery were recruited sequentially into two cohorts: cohort 1 received oral atovaquone at the standard clinical dose of 750 mg twice daily, while cohort 2 did not. Primary imaging endpoint was change in tumor hypoxic volume (HV) measured by hypoxia PET-CT. Intercohort comparison of hypoxia gene expression signatures using RNA sequencing from resected tumors was performed.
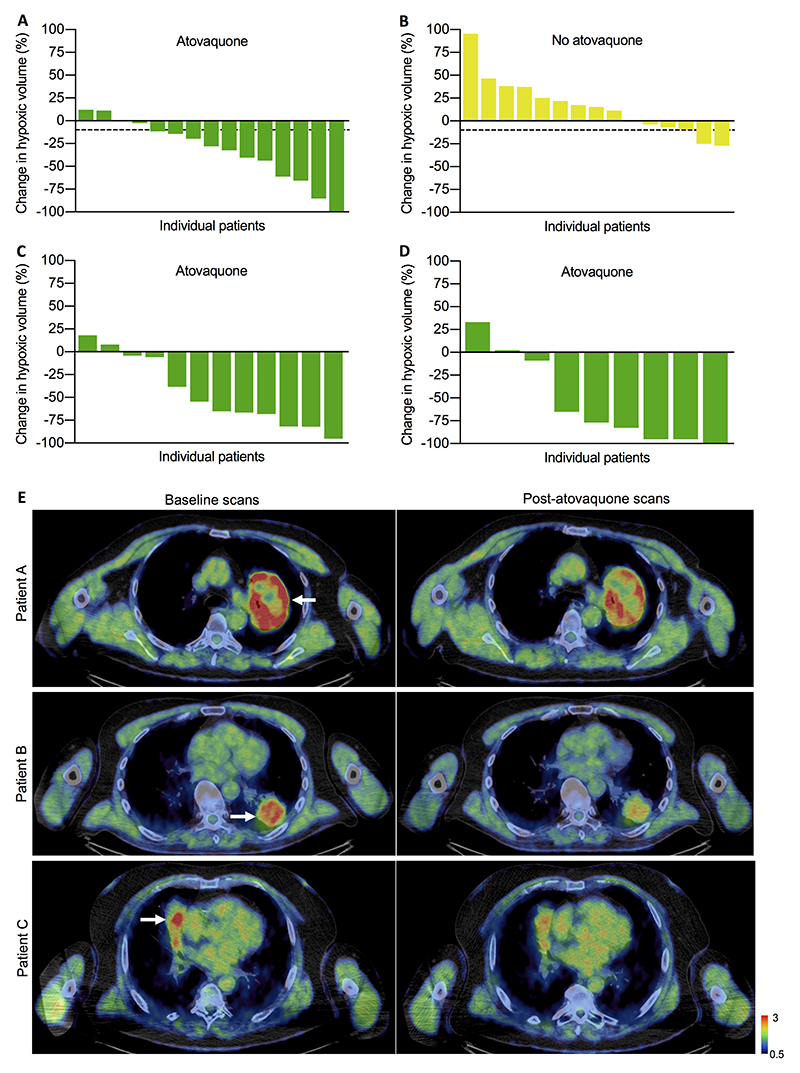
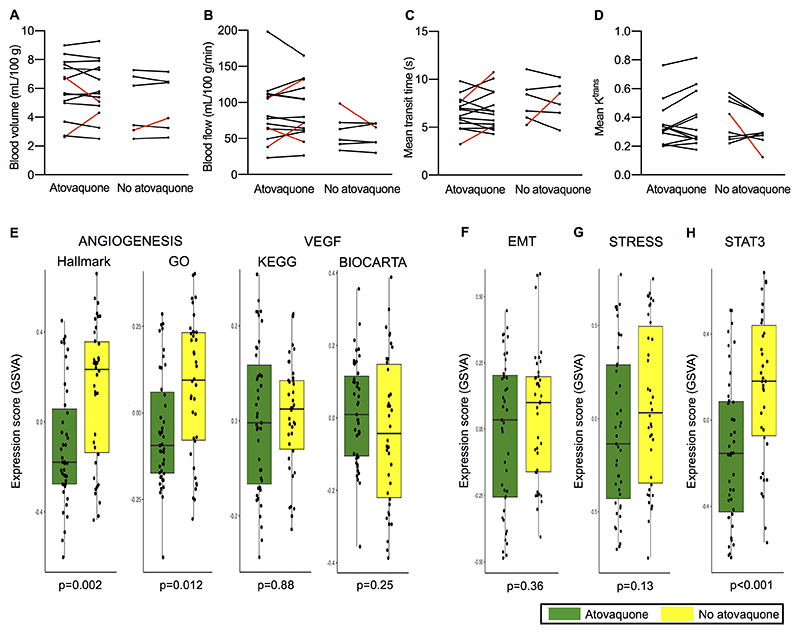
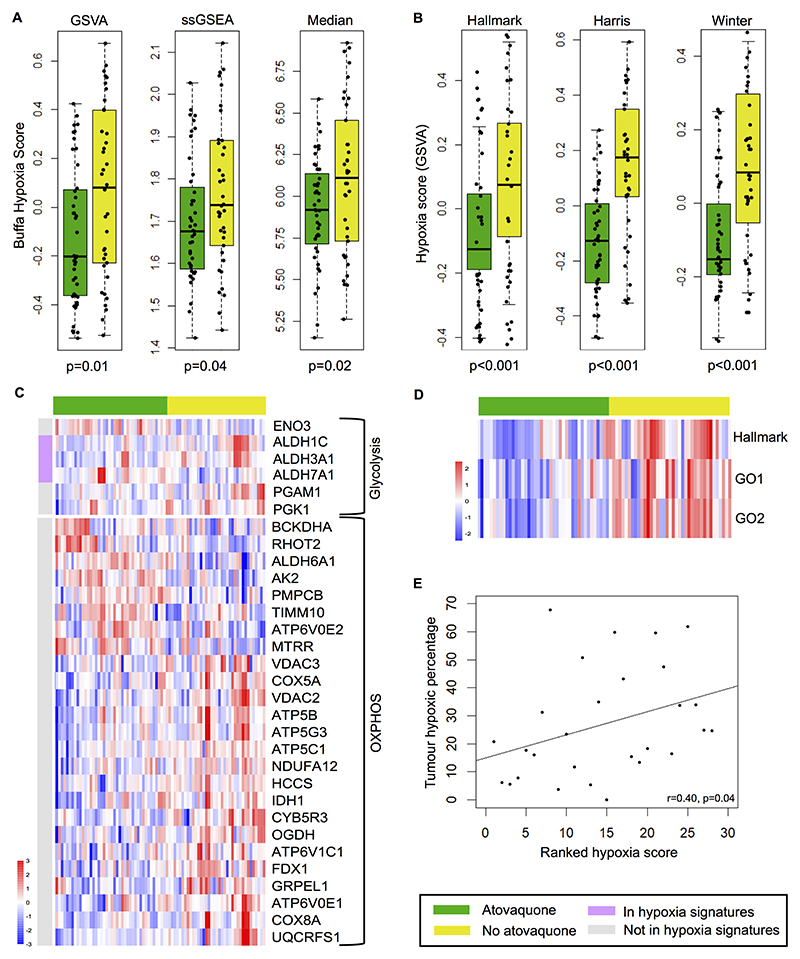
Thirty patients were evaluable for hypoxia PET-CT analysis, 15 per cohort. Median treatment duration was 12 days. Eleven (73.3%) atovaquone-treated patients had meaningful HV reduction, with median change -28% [95% confidence interval (CI), -58.2 to -4.4]. In contrast, median change in untreated patients was +15.5% (95% CI, -6.5 to 35.5). Linear regression estimated the expected mean HV was 55% (95% CI, 24%-74%) lower in cohort 1 compared with cohort 2 ( = 0.004), adjusting for cohort, tumor volume, and baseline HV. A key pharmacodynamics endpoint was reduction in hypoxia-regulated genes, which were significantly downregulated in atovaquone-treated tumors. Data from multiple additional measures of tumor hypoxia and perfusion are presented. No atovaquone-related adverse events were reported.
This is the first clinical evidence that targeting tumor mitochondrial metabolism can reduce hypoxia and produce relevant antitumor effects at the mRNA level. Repurposing atovaquone for this purpose may improve treatment outcomes for NSCLC.
肿瘤缺氧会促进侵袭性肿瘤表型的形成,并导致对癌症治疗的耐药性。我们进行了一项临床试验,以确定抗疟药物阿托伐醌(一种已知的线粒体抑制剂)是否能降低非小细胞肺癌(NSCLC)的缺氧程度。
计划接受手术的 NSCLC 患者被连续纳入两个队列:队列 1 患者接受标准临床剂量的阿托伐醌(750 mg,每日 2 次),而队列 2 患者未接受阿托伐醌治疗。主要影像学终点是通过缺氧 PET-CT 测量肿瘤缺氧体积(HV)的变化。对切除肿瘤的 RNA 测序进行了缺氧基因表达谱的组间比较。
30 例患者可进行缺氧 PET-CT 分析,每个队列 15 例。中位治疗时间为 12 天。11 例(73.3%)接受阿托伐醌治疗的患者 HV 有明显减少,中位变化为-28%(95%置信区间 [CI],-58.2 至-4.4)。相比之下,未接受治疗的患者的中位变化为+15.5%(95% CI,-6.5 至 35.5)。线性回归估计,与队列 2 相比,队列 1 中 HV 的预期平均水平预计将低 55%(95% CI,24%-74%)( = 0.004),调整了队列、肿瘤体积和基线 HV。一个关键的药效学终点是缺氧调节基因的减少,阿托伐醌治疗的肿瘤中这些基因显著下调。还报告了来自多个肿瘤缺氧和灌注的额外测量结果。未报告与阿托伐醌相关的不良反应。
这是首个临床证据表明,靶向肿瘤线粒体代谢可以降低缺氧程度,并在 mRNA 水平上产生相关的抗肿瘤作用。将阿托伐醌重新用于该目的可能会改善 NSCLC 的治疗效果。