Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina, USA.
Department of Pediatrics, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, North Carolina, USA.
Health Serv Res. 2021 Oct;56(5):864-873. doi: 10.1111/1475-6773.13641. Epub 2021 Feb 17.
To improve food insecurity interventions, we sought to better understand the hypothesized bidirectional relationship between food insecurity and health care expenditures.
Nationally representative sample of the civilian noninstitutionalized population of the United States (2016-2017 Medical Expenditure Panel Survey [MEPS]).
In a retrospective longitudinal cohort, we conducted two sets of analyses: (a) two-part models to examine the association between food insecurity in 2016 and health care expenditures in 2017; and (b) logistic regression models to examine the association between health care expenditures in 2016 and food insecurity in 2017. We adjusted for demographic and socioeconomic variables as well as 2016 health care expenditures and food insecurity.
Health care expenditures, food insecurity, and medical condition data from 10 886 adults who were included in 2016-2017 MEPS.
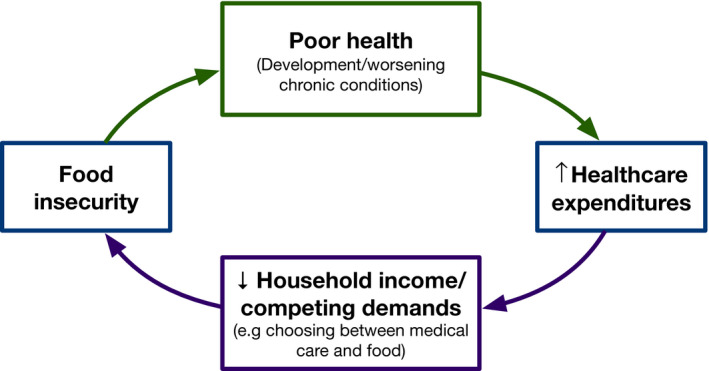
Food insecurity in 2016, compared with being food secure, was associated with both a higher odds of having any health care expenditures in 2017 (OR 1.29, 95% CI: 1.04 to 1.60) and greater total expenditures ($1738.88 greater, 95% CI: $354.10 to $3123.57), which represents approximately 25% greater expenditures. Greater 2016 health care expenditures were associated with slightly higher odds of being food insecure in 2017 (OR 1.007 per $1000 in expenditures, 95% CI: 1.002 to 1.012, P =0.01). Exploratory analyses suggested that poor health status may underlie the relationship between food insecurity and health care expenditures.
A bidirectional relationship exists between food insecurity and health care expenditures, but the strength of either direction appears unequal. Higher health care expenditures are associated with a slightly greater risk of being food insecure (adjusted for baseline food insecurity status) but being food insecure is associated with substantially greater subsequent health care expenditures (adjusted for baseline health care expenditures). Interventions to address food insecurity and poor health may be helpful to break this cycle.
为了改善粮食不安全干预措施,我们试图更好地理解粮食不安全和医疗支出之间假定的双向关系。
美国平民非机构人口的全国代表性样本(2016-2017 年医疗支出面板调查 [MEPS])。
在回顾性纵向队列中,我们进行了两组分析:(a)两部分模型,以检验 2016 年粮食不安全与 2017 年医疗支出之间的关联;(b)逻辑回归模型,以检验 2016 年医疗支出与 2017 年粮食不安全之间的关联。我们调整了人口统计学和社会经济变量以及 2016 年的医疗支出和粮食不安全状况。
来自 10886 名成年人的数据,这些成年人在 2016-2017 年 MEPS 中被纳入,包括医疗支出、粮食不安全和医疗状况数据。
与粮食安全相比,2016 年粮食不安全与 2017 年任何医疗支出的可能性更高(比值比 1.29,95%置信区间:1.04 至 1.60)和总支出更高(高出$1738.88,95%置信区间:$354.10 至 $3123.57),这代表支出增加约 25%。2016 年较高的医疗支出与 2017 年粮食不安全的可能性略高相关(每 1000 美元支出增加 1.007 美元,95%置信区间:1.002 至 1.012,P=0.01)。探索性分析表明,粮食不安全与医疗支出之间的关系可能源于健康状况不佳。
粮食不安全和医疗支出之间存在双向关系,但任何一个方向的强度似乎都不平等。较高的医疗支出与略高的粮食不安全风险相关(调整基线粮食不安全状况),但粮食不安全与随后的医疗支出显著增加相关(调整基线医疗支出)。解决粮食不安全和健康状况不佳问题的干预措施可能有助于打破这一循环。