Division of Cardiology, Department of Cardiovascular Diseases, Cliniques Universitaires St. Luc and Pôle de Recherche Cardiovasculaire (CARD), Institut de Recherche Expérimentale et Clinique (IREC), Cardiovascular Division, Université Catholique de Louvain, Avenue Hippocrate, 10, 1200, Brussels, Belgium.
Cardiovasc Diabetol. 2021 Feb 19;20(1):48. doi: 10.1186/s12933-021-01242-5.
Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous syndrome, with several underlying etiologic and pathophysiologic factors. The presence of diabetes might identify an important phenotype, with implications for therapeutic strategies. While diabetes is associated with worse prognosis in HFpEF, the prognostic impact of glycemic control is yet unknown. Hence, we investigated phenotypic differences between diabetic and non-diabetic HFpEF patients (pts), and the prognostic impact of glycated hemoglobin (HbA1C).
We prospectively enrolled 183 pts with HFpEF (78 ± 9 years, 38% men), including 70 (38%) diabetics (type 2 diabetes only). They underwent 2D echocardiography (n = 183), cardiac magnetic resonance (CMR) (n = 150), and were followed for a combined outcome of all-cause mortality and first HF hospitalization. The prognostic impact of diabetes and glycemic control were determined with Cox proportional hazard models, and illustrated by adjusted Kaplan Meier curves.
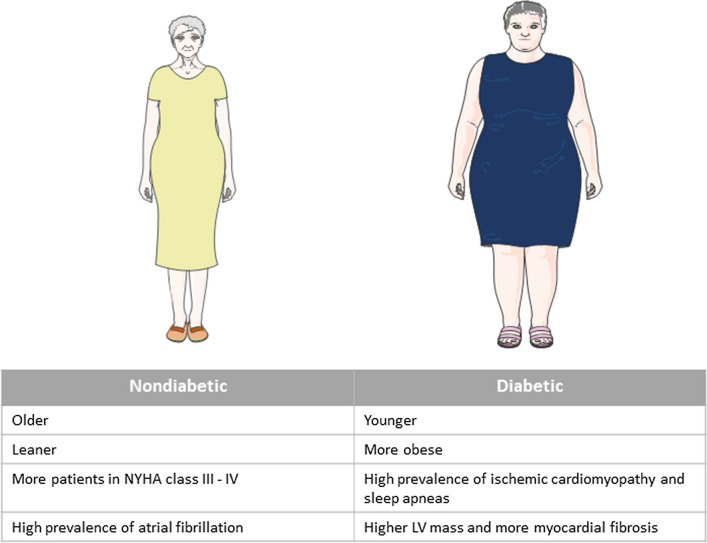
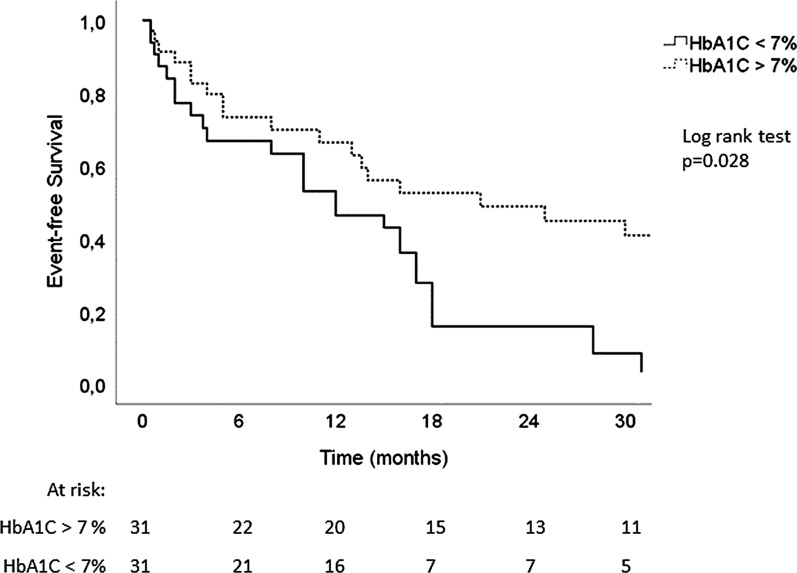
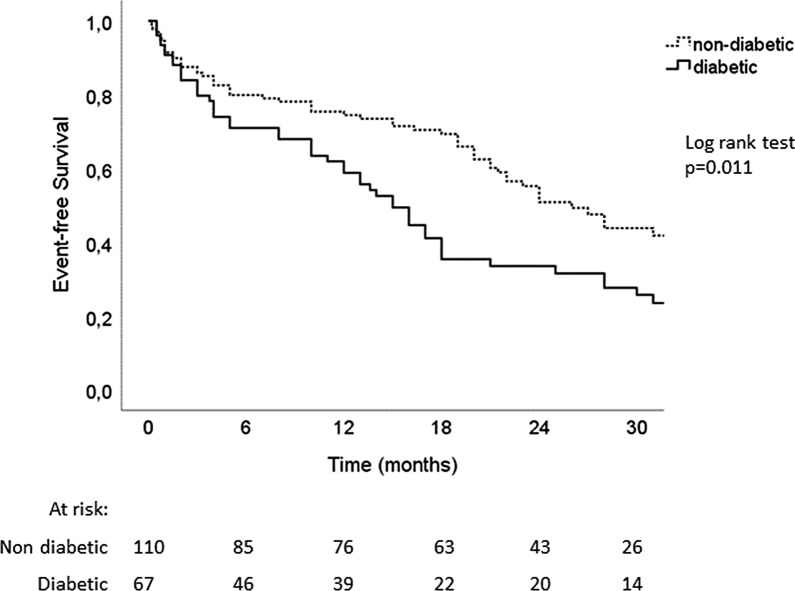
Diabetic HFpEF pts were younger (76 ± 9 vs 80 ± 8 years, p = 0.002), more obese (BMI 31 ± 6 vs 27 ± 6 kg/m, p = 0.001) and suffered more frequently from sleep apnea (18% vs 7%, p = 0.032). Atrial fibrillation, however, was more frequent in non-diabetic pts (69% vs 53%, p = 0.028). Although no echocardiographic difference could be detected, CMR analysis revealed a trend towards higher LV mass (66 ± 18 vs 71 ± 14 g/m, p = 0.07) and higher levels of fibrosis (53% vs 36% of patients had ECV by T1 mapping > 33%, p = 0.05) in diabetic patients. Over 25 ± 12 months, 111 HFpEF pts (63%) reached the combined outcome (24 deaths and 87 HF hospitalizations). Diabetes was a significant predictor of mortality and hospitalization for heart failure (HR: 1.72 [1.1-2.6], p = 0.011, adjusted for age, BMI, NYHA class and renal function). In diabetic patients, lower levels of glycated hemoglobin (HbA1C < 7%) were associated with worse prognosis (HR: 2.07 [1.1-4.0], p = 0.028 adjusted for age, BMI, hemoglobin and NT-proBNP levels).
Our study highlights phenotypic features characterizing diabetic patients with HFpEF. Notably, they are younger and more obese than their non-diabetic counterpart, but suffer less from atrial fibrillation. Although diabetes is a predictor of poor outcome in HFpEF, intensive glycemic control (HbA1C < 7%) in diabetic patients is associated with worse prognosis.
射血分数保留的心力衰竭(HFpEF)是一种异质性综合征,存在多种潜在的病因和病理生理因素。糖尿病的存在可能会识别出一个重要的表型,这对治疗策略有影响。虽然糖尿病与 HFpEF 的预后较差相关,但血糖控制的预后影响尚不清楚。因此,我们研究了糖尿病和非糖尿病 HFpEF 患者(pts)之间的表型差异,以及糖化血红蛋白(HbA1C)的预后影响。
我们前瞻性纳入了 183 例 HFpEF 患者(78±9 岁,38%为男性),其中 70 例(38%)为糖尿病患者(仅 2 型糖尿病)。他们接受了 2 维超声心动图(n=183)、心脏磁共振(CMR)(n=150)检查,并随访了所有原因死亡和首次 HF 住院的复合结局。使用 Cox 比例风险模型确定糖尿病和血糖控制的预后影响,并通过调整后的 Kaplan-Meier 曲线进行说明。
糖尿病 HFpEF 患者更年轻(76±9 岁 vs 80±8 岁,p=0.002),更肥胖(BMI 31±6 千克/平方米 vs 27±6 千克/平方米,p=0.001),更常患有睡眠呼吸暂停(18% vs 7%,p=0.032)。然而,非糖尿病患者中房颤更为常见(69% vs 53%,p=0.028)。尽管在超声心动图上没有发现差异,但 CMR 分析显示,糖尿病患者的左心室质量(66±18 克/平方米 vs 71±14 克/平方米,p=0.07)和纤维化水平(53%的患者通过 T1 映射的 ECV>33%,而 36%的患者,p=0.05)呈上升趋势。在 25±12 个月的随访中,111 例 HFpEF 患者(63%)达到了复合结局(24 例死亡和 87 例 HF 住院)。糖尿病是死亡和心力衰竭住院的显著预测因素(HR:1.72 [1.1-2.6],p=0.011,调整了年龄、BMI、NYHA 分级和肾功能)。在糖尿病患者中,糖化血红蛋白(HbA1C<7%)水平较低与预后较差相关(HR:2.07 [1.1-4.0],p=0.028,调整了年龄、BMI、血红蛋白和 NT-proBNP 水平)。
我们的研究强调了糖尿病 HFpEF 患者的表型特征。值得注意的是,与非糖尿病患者相比,他们更年轻、更肥胖,但房颤发病率较低。尽管糖尿病是 HFpEF 不良预后的预测因素,但糖尿病患者强化血糖控制(HbA1C<7%)与预后较差相关。