MRC Institute of Genetic and Molecular Medicine, University of Edinburgh, Edinburgh, UK.
Division of Molecular and Clinical Medicine, University of Dundee, Dundee, UK.
Diabetologia. 2021 Jun;64(6):1309-1319. doi: 10.1007/s00125-021-05394-7. Epub 2021 Feb 19.
AIMS/HYPOTHESIS: The aim of this work was to map the number of prescribed drugs over age, sex and area-based socioeconomic deprivation, and to examine the association between the number of drugs and particular high-risk drug classes with adverse health outcomes among a national cohort of individuals with type 1 diabetes.
Utilising linked healthcare records from the population-based diabetes register of Scotland, we identified 28,245 individuals with a diagnosis of type 1 diabetes on 1 January 2017. For this population, we obtained information on health status, predominantly reflecting diabetes-related complications, and information on the total number of drugs and particular high-risk drug classes prescribed. We then studied the association of these baseline-level features with hospital admissions for falls, diabetic ketoacidosis (DKA), and hypoglycaemia or death within the subsequent year using multivariate Cox proportional hazards models.
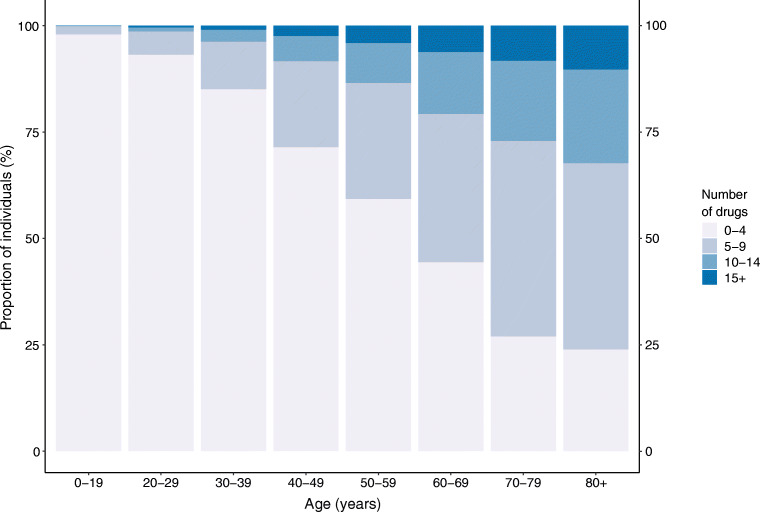
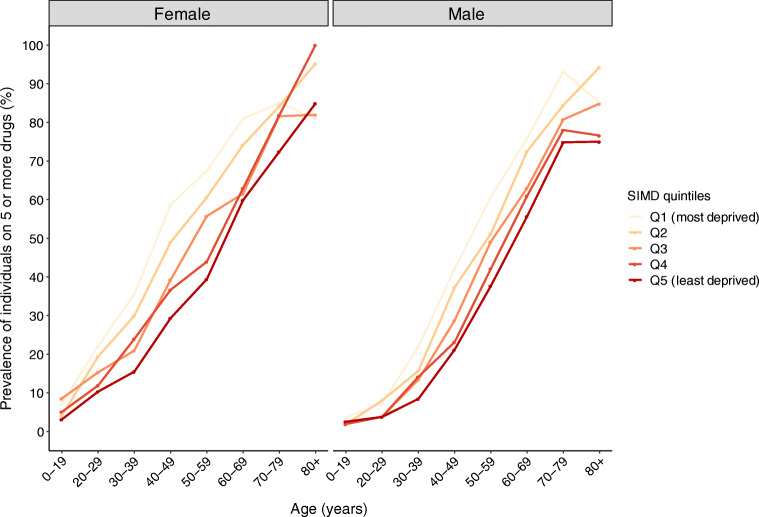
Not considering insulin and treatment for hypoglycaemia, the mean number of prescribed drugs was 4.00 (SD 4.35). The proportion of individuals being prescribed five or more drugs at baseline consistently increased with age (proportion [95% CI]: 0-19 years 2.04% [1.60, 2.49]; 40-49 years 28.50% [27.08, 29.93]; 80+ years 76.04% [67.73, 84.84]). Controlling for age, sex, area-based socioeconomic deprivation and health status, each additional drug at baseline was associated with an increase in the hazard for hospitalisation for falls, hypoglycaemia and death but not for DKA admissions (HR [95% CI]: falls 1.03 [1.01, 1.06]; DKA 1.01 [1.00, 1.03]; hypoglycaemia 1.05 [1.02, 1.07]; death 1.04 [1.02, 1.06]). We found a number of drug classes to be associated with an increased hazard of one or more of these adverse health outcomes, including antithrombotic/anticoagulant agents, corticosteroids, opioids, antiepileptics, antipsychotics, hypnotics and sedatives, and antidepressants.
Polypharmacy is common among the Scottish population with type 1 diabetes and is strongly patterned by sociodemographic factors. The number of prescribed drugs and the prescription of particular high-risk drug classes are strong markers of an increased risk of adverse health outcomes, including acute complications of diabetes.
目的/假设:本研究旨在绘制按年龄、性别和基于地区的社会经济剥夺程度划分的处方药数量,并研究在苏格兰基于人群的糖尿病登记处的全国队列中,特定高危药物类别与不良健康结果之间的数量与药物之间的关联患有 1 型糖尿病的个体。
我们利用苏格兰基于人群的糖尿病登记处的连锁医疗记录,确定了 2017 年 1 月 1 日患有 1 型糖尿病的 28,245 名个体。对于该人群,我们获得了健康状况的信息,主要反映了糖尿病相关并发症,以及处方的总药物数量和特定高危药物类别的信息。然后,我们使用多变量 Cox 比例风险模型研究了这些基线特征与随后一年内因跌倒、糖尿病酮症酸中毒 (DKA)、低血糖或死亡而住院之间的关联。
不考虑胰岛素和低血糖治疗,处方药物的平均数量为 4.00(SD 4.35)。在基线时,开具五种或更多药物的个体比例随着年龄的增长而持续增加(比例[95%CI]:0-19 岁 2.04%[1.60,2.49];40-49 岁 28.50%[27.08,29.93];80+岁 76.04%[67.73,84.84])。控制年龄、性别、基于地区的社会经济剥夺和健康状况后,基线时每增加一种药物与跌倒、低血糖和死亡住院风险增加相关,但与 DKA 入院无关(HR[95%CI]:跌倒 1.03[1.01,1.06];DKA 1.01[1.00,1.03];低血糖 1.05[1.02,1.07];死亡 1.04[1.02,1.06])。我们发现许多药物类别与这些不良健康结果中的一种或多种的发生风险增加有关,包括抗血栓/抗凝药物、皮质类固醇、阿片类药物、抗癫痫药、抗精神病药、催眠药和镇静剂以及抗抑郁药。
苏格兰 1 型糖尿病人群普遍存在多药治疗,且受社会人口因素的强烈影响。处方药数量和特定高危药物类别的处方是不良健康结果风险增加的有力标志物,包括糖尿病急性并发症。