Division of Molecular Pathology, The Netherlands Cancer Institute, Amsterdam, The Netherlands.
Institute of Biostatistics and Registry Research, Brandenburg Medical School Theodor Fontane, Neuruppin, Germany.
J Pathol Clin Res. 2021 May;7(3):233-242. doi: 10.1002/cjp2.201. Epub 2021 Feb 23.
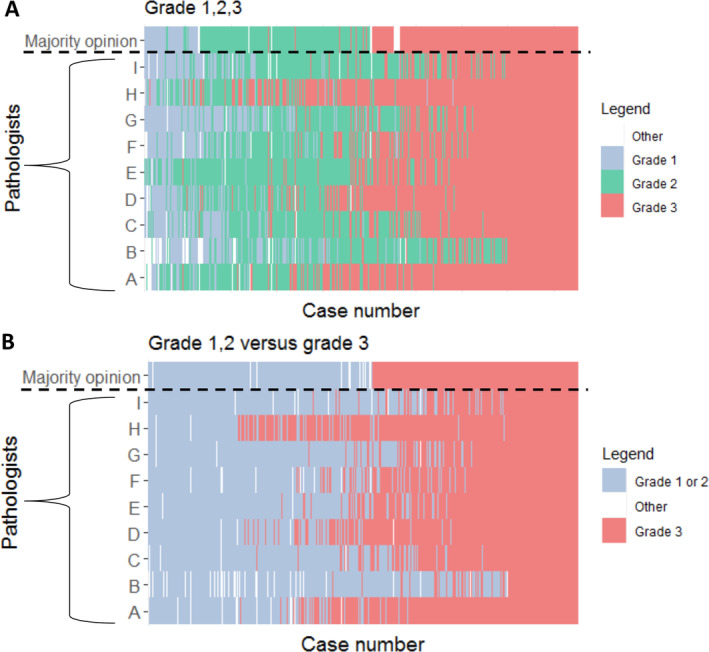
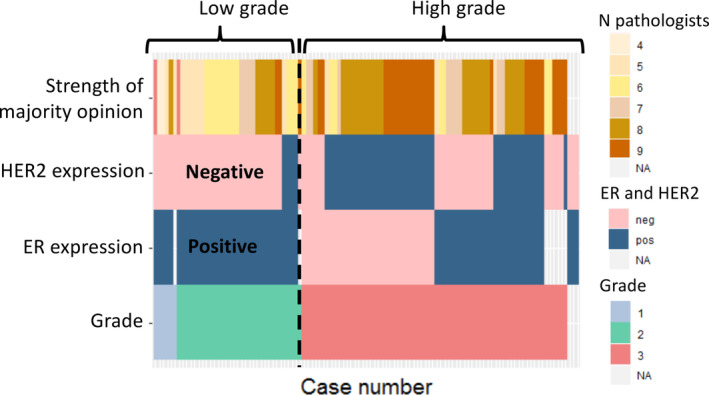
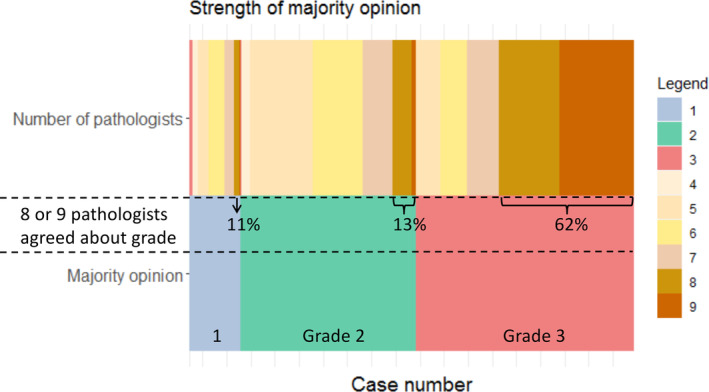
The prognostic value of cytonuclear grade in ductal carcinoma in situ (DCIS) is debated, partly due to high interobserver variability and the use of multiple guidelines. The aim of this study was to evaluate interobserver agreement in grading DCIS between Dutch, British, and American pathologists. Haematoxylin and eosin-stained slides of 425 women with primary DCIS were independently reviewed by nine breast pathologists based in the Netherlands, the UK, and the USA. Chance-corrected kappa (κ ) for association between pathologists was calculated based on a generalised linear mixed model using the ordinal package in R. Overall κ for grade of DCIS (low, intermediate, or high) was estimated to be 0.50 (95% confidence interval [CI] 0.44-0.56), indicating a moderate association between pathologists. When the model was adjusted for national guidelines, the association for grade did not change (κ = 0.53; 95% CI 0.48-0.57); subgroup analysis for pathologists using the UK pathology guidelines only had significantly higher association (κ = 0.58; 95% CI 0.56-0.61). To assess if concordance of grading relates to the expression of the oestrogen receptor (ER) and HER2, archived immunohistochemistry was analysed on a subgroup (n = 106). This showed that non-high grade according to the majority opinion was associated with ER positivity and HER2 negativity (100 and 89% of non-high grade cases, respectively). In conclusion, DCIS grade showed only moderate association using whole slide images scored by nine breast pathologists. As therapeutic decisions and inclusion in ongoing clinical trials are guided by DCIS grade, there is a pressing need to reduce interobserver variability in grading. ER and HER2 might be supportive to prevent the accidental and unwanted inclusion of high-grade DCIS in such trials.
核型分级在导管原位癌(DCIS)中的预后价值存在争议,部分原因是观察者间的变异性较大,以及使用了多种指南。本研究旨在评估荷兰、英国和美国的病理学家在 DCIS 分级方面的观察者间一致性。对 425 名原发性 DCIS 女性的苏木精和伊红染色切片,由荷兰、英国和美国的 9 名乳腺病理学家进行独立评估。基于 R 语言中的 ordinal 包,使用广义线性混合模型计算病理学家之间的等级关联的校正机遇kappa(κ)。DCIS 分级(低、中或高)的总体κ值估计为 0.50(95%置信区间 0.44-0.56),表明病理学家之间存在中度关联。当模型根据国家指南进行调整时,分级的关联没有改变(κ=0.53;95%置信区间 0.48-0.57);仅使用英国病理指南的病理学家的亚组分析显示出显著更高的关联(κ=0.58;95%置信区间 0.56-0.61)。为了评估分级的一致性是否与雌激素受体(ER)和 HER2 的表达有关,对一个亚组(n=106)的存档免疫组化进行了分析。这表明,根据多数意见,非高级别与 ER 阳性和 HER2 阴性相关(分别为 100%和 89%的非高级别病例)。总之,使用 9 名乳腺病理学家评估全切片图像时,DCIS 分级仅显示出中度的相关性。由于 DCIS 分级指导着治疗决策和纳入正在进行的临床试验,因此迫切需要减少分级方面的观察者间变异性。ER 和 HER2 可能有助于防止在这些试验中意外和不必要地纳入高级别 DCIS。