Department of Pathology, Cliniques universitaires Saint-Luc, Avenue Hippocrate 10, 1200, Brussels, Belgium.
Pôle de Morphologie (MORF), Institut de Recherche Expérimentale et Clinique, Université catholique de Louvain, Avenue Hippocrate 10, 1200, Brussels, Belgium.
Breast Cancer Res. 2024 Aug 27;26(1):125. doi: 10.1186/s13058-024-01875-w.
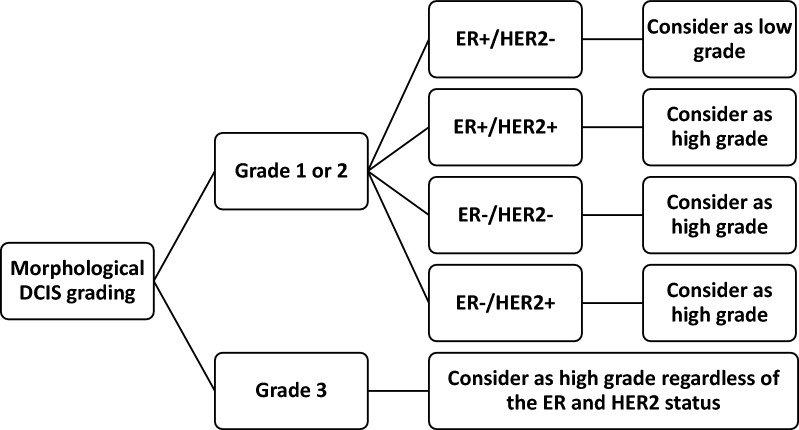
In many countries, hormone receptor status assessment of ductal carcinoma in situ (DCIS) is routinely performed, as hormone receptor-positive DCIS patients are eligible for adjuvant anti-hormonal treatment, aiming to reduce the ipsilateral and contralateral breast cancer risk. Although HER2 gene amplification and its associated HER2 protein overexpression constitute a major prognostic and predictive marker in invasive breast carcinoma, its use in the diagnosis and treatment of DCIS is less straightforward. HER2 immunohistochemistry is not routinely performed yet, as the role of HER2-positivity in DCIS biology is unclear. Nonetheless, recent data challenge this practice. Here, we discuss the value of routine HER2 assessment for DCIS. HER2-positivity correlates strongly with DCIS grade: around four in five HER2-positive DCIS show high grade atypia. As morphological DCIS grading is prone to interobserver variability, HER2 immunohistochemistry could render grading more robust. Several studies showed an association between HER2-positive DCIS and ipsilateral recurrence risk, albeit currently unclear whether this is for overall, in situ or invasive recurrence. HER2-positive DCIS tends to be larger, with a higher risk of involved surgical margins. HER2-positive DCIS patients benefit more from adjuvant radiotherapy: it substantially decreases the local recurrence risk after lumpectomy, without impact on overall survival. HER2-positivity in pure biopsy-diagnosed DCIS is associated with increased upstaging to invasive carcinoma after surgery. HER2 immunohistochemistry on preoperative biopsies might therefore provide useful information to surgeons, favoring wider excisions. The time seems right to consider DCIS subtype-dependent treatment, comprising appropriate local treatment for HER2-positive DCIS patients and de-escalation for hormone receptor-positive, HER2-negative DCIS patients.
在许多国家,导管原位癌(DCIS)的激素受体状态评估通常是常规进行的,因为激素受体阳性的 DCIS 患者有资格接受辅助抗激素治疗,旨在降低同侧和对侧乳腺癌的风险。虽然 HER2 基因扩增及其相关的 HER2 蛋白过表达是浸润性乳腺癌的主要预后和预测标志物,但它在 DCIS 的诊断和治疗中的应用并不那么直接。HER2 免疫组化尚未常规进行,因为 HER2 阳性在 DCIS 生物学中的作用尚不清楚。尽管如此,最近的数据对这一做法提出了挑战。在这里,我们讨论了常规 HER2 评估在 DCIS 中的价值。HER2 阳性与 DCIS 分级密切相关:约五分之四的 HER2 阳性 DCIS 显示高级别异型性。由于形态学 DCIS 分级容易受到观察者间的差异,HER2 免疫组化可以使分级更可靠。几项研究表明,HER2 阳性 DCIS 与同侧复发风险之间存在关联,尽管目前尚不清楚这是针对总体、原位还是浸润性复发。HER2 阳性 DCIS 往往更大,手术切缘受累的风险更高。HER2 阳性 DCIS 患者从辅助放疗中获益更多:它显著降低了保乳手术后的局部复发风险,而对总生存没有影响。在纯活检诊断的 DCIS 中,HER2 阳性与手术后向浸润性癌升级增加有关。因此,术前活检的 HER2 免疫组化可能为外科医生提供有用的信息,有利于更广泛的切除。现在似乎是考虑基于 DCIS 亚型的治疗的时候了,包括对 HER2 阳性 DCIS 患者进行适当的局部治疗,对激素受体阳性、HER2 阴性的 DCIS 患者进行降级治疗。