Institute of Inflammation and Ageing, University of Birmingham College of Medical and Dental Sciences, Birmingham, UK
Department of Neurosurgery, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
BMJ Open. 2021 Feb 23;11(2):e047063. doi: 10.1136/bmjopen-2020-047063.
To determine how the first wave of the COVID-19 pandemic affected outcomes for all operatively managed neurosurgical patients, not only those positive for SARS-CoV-2.
Matched cohort (pairwise method).
A single tertiary neurosurgical referral centre at a large UK Major Trauma Centre.
During the first COVID-19 wave, 231 neurosurgical cases were performed. These cases were matched to cases from 2019. Cases were matched for age (±10 years), primary pathology and surgical procedure. Cases were excluded from analysis if either the age could not be matched to within 10 years, or the primary pathology or procedure was too unique. After exclusions, 191 cases were included in final analysis.
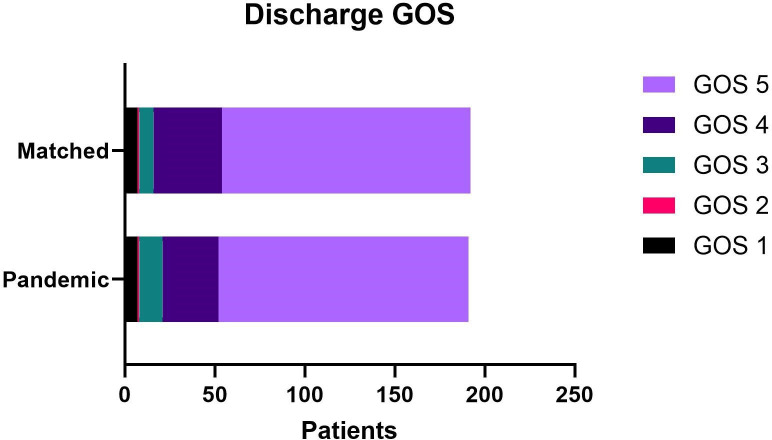
Primary outcomes were 30-day mortality and postoperative pulmonary complications. Secondary outcomes included Glasgow Outcome Score (GOS) on discharge, length of stay (LoS), operative and anaesthetic times and grade of primary surgeon. An exploratory outcome was the SARS-CoV-2 status of patients.
There was no significant difference between the pandemic and matched cohorts in 30-day mortality, pulmonary complications, discharge GOS, LoS, operative or anaesthetic times. There was a significant difference in the variation of grade of primary surgeon. Only 2.2% (n=5) of patients had a SARS-CoV-2 positive swab.
During the first UK wave of the COVID-19 pandemic, the mortality, morbidity and functional outcomes of operatively managed neurosurgical patients at University Hospitals Birmingham were not significantly affected compared with normal practice. The grade of primary surgeon was significantly more senior and adds to the growing body of evidence that demonstrates how the pandemic has negatively impacted UK surgical training. Mixing COVID-19 positive, unknown and negative cases did not significantly impact on outcomes and indicates that further research is required to support the implementation of evidence-based surgical pathways, such as COVID-light sites, throughout the next stage of the pandemic.
确定 COVID-19 大流行的第一波如何影响所有接受手术治疗的神经外科患者的结局,而不仅仅是那些 SARS-CoV-2 阳性的患者。
匹配队列(成对法)。
英国大型创伤中心的一家单一三级神经外科转诊中心。
在 COVID-19 大流行的第一波期间,进行了 231 例神经外科手术。这些病例与 2019 年的病例相匹配。病例按年龄(±10 岁)、主要病理和手术程序进行匹配。如果年龄无法匹配 10 岁以内,或者主要病理或手术程序过于独特,则将病例排除在分析之外。排除后,191 例纳入最终分析。
主要结果是 30 天死亡率和术后肺部并发症。次要结果包括出院时的格拉斯哥结局评分(GOS)、住院时间(LoS)、手术和麻醉时间以及主刀医生的级别。一个探索性结果是患者的 SARS-CoV-2 状态。
在 30 天死亡率、肺部并发症、出院 GOS、LoS、手术或麻醉时间方面,大流行组与匹配组之间没有显著差异。主刀医生级别的变化有显著差异。只有 2.2%(n=5)的患者 SARS-CoV-2 拭子检测呈阳性。
在 COVID-19 大流行的第一波期间,伯明翰大学医院接受手术治疗的神经外科患者的死亡率、发病率和功能结局与常规治疗相比没有显著影响。主刀医生的级别明显更高,这进一步证明了大流行如何对英国外科培训产生负面影响。混合 COVID-19 阳性、未知和阴性病例对结局没有显著影响,这表明需要进一步研究以支持在大流行的下一阶段实施基于证据的外科途径,如 COVID-轻站点。