Fotheringham James, Latimer Nicholas, Froissart Marc, Kronenberg Florian, Stenvinkel Peter, Floege Jürgen, Eckardt Kai-Uwe, Wheeler David C
Sheffield Kidney Institute, Sheffield Teaching Hospitals, Sheffield, UK.
School of Health and Related Research, University of Sheffield, Sheffield, UK.
Clin Kidney J. 2020 Dec 28;14(2):665-672. doi: 10.1093/ckj/sfaa250. eCollection 2021 Feb.
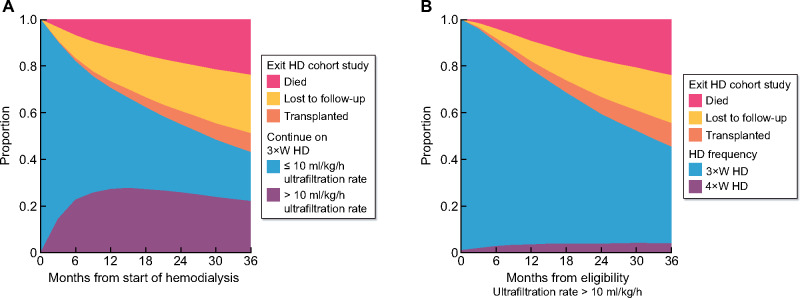
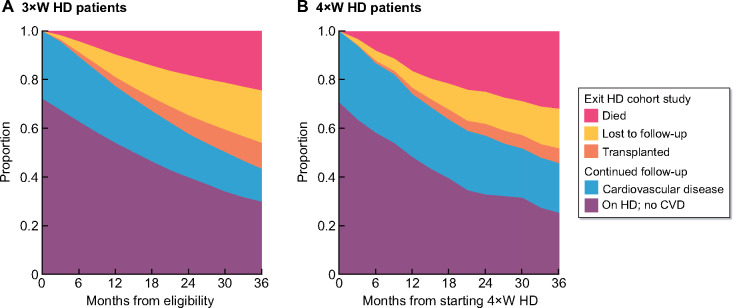
The harm caused by the long interdialytic interval in three-times-per-week haemodialysis regimens (3×WHD) may relate to fluid accumulation and associated high ultrafiltration rate (UFR). Four-times-per-week haemodialysis (4×WHD) may offer a solution, but its impact on mortality, hospitalization and vascular access complications is unknown.
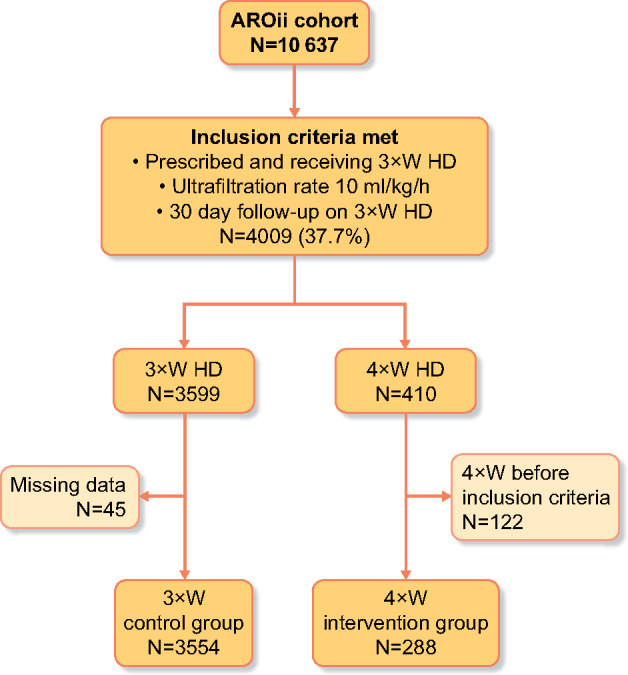
From the AROii cohort of incident in-centre haemodialysis patients, 3×WHD patients with a UFR >10 mL/kg/h were identified. The hazard for the outcomes of mortality, hospitalization and vascular access complications in those who switched to 4×WHD compared with staying on 3×WHD was estimated using a marginal structural Cox proportional hazards model. Adjustment included baseline patient and treatment characteristics with inverse probability weighting used to adjust for time-varying UFR and cardiovascular comorbidities.
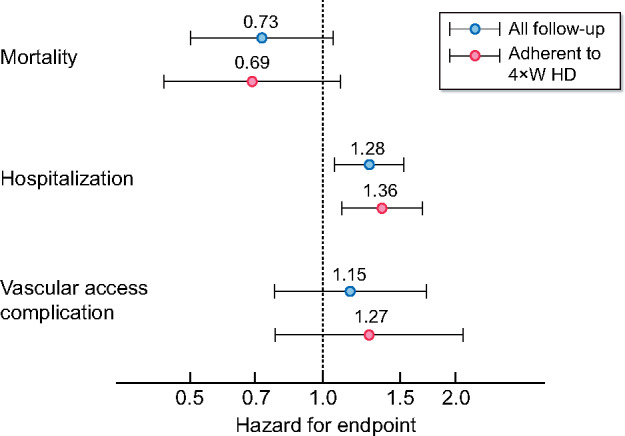
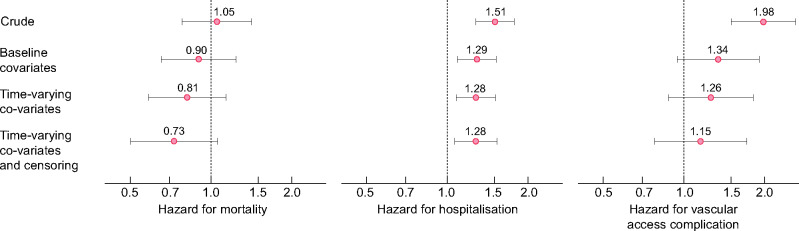
From 10 637 European 3×WHD patients, 3842 (36%) exceeded a UFR >10 mL/kg/h. Of these, 288 (7.5%) started 4×WHD and at baseline were more comorbid. Event rates while receiving 4×WHD compared with 3×WHD were 12.6 compared with 10.8 per 100 patient years for mortality, 0.96 compared with 0.65 per year for hospitalization and 14.7 compared with 8.0 per 100 patient years for vascular access complications. Compared with 3×WHD, the unadjusted hazard ratio (HR) for mortality on 4×WHD was 1.05 [95% confidence interval (CI) 0.78-1.42]. Following adjustment for baseline demographics, time-varying treatment probability and censoring risks, this HR was 0.73 (95% CI 0.50-1.05; P = 0.095). Despite these adjustments on 4×WHD, the HR for hospitalization remained elevated and vascular access complications were similar to 3×WHD.
This observational study was not able to demonstrate a mortality benefit in patients switched to 4×WHD. To demonstrate the true benefits of 4×WHD requires a large, well-designed clinical trial. Our data may help in the design of such a study.
每周三次血液透析方案(3×WHD)中透析间期过长所造成的危害可能与液体潴留及相关的高超滤率(UFR)有关。每周四次血液透析(4×WHD)或许能提供一种解决方案,但其对死亡率、住院率及血管通路并发症的影响尚不清楚。
从AROii队列中纳入新发的中心血液透析患者,确定超滤率>10 mL/kg/h的3×WHD患者。使用边际结构Cox比例风险模型估计那些转为4×WHD的患者与继续接受3×WHD的患者相比,在死亡率、住院率及血管通路并发症方面的风险。调整因素包括患者基线特征和治疗特征,采用逆概率加权法调整随时间变化的超滤率和心血管合并症。
在10637例欧洲3×WHD患者中,3842例(36%)超滤率>10 mL/kg/h。其中,288例(7.5%)开始接受4×WHD,且在基线时合并症更多。接受4×WHD与3×WHD相比,每100患者年的死亡率分别为12.6和10.8,住院率分别为每年0.96和0.65,血管通路并发症分别为每100患者年14.7和8.0。与3×WHD相比,4×WHD未调整的死亡风险比(HR)为1.05 [95%置信区间(CI)0.78 - 1.42]。在对基线人口统计学、随时间变化的治疗概率和删失风险进行调整后,该HR为0.73(95% CI 0.50 - 1.05;P = 0.095)。尽管对4×WHD进行了这些调整,但其住院HR仍升高,且血管通路并发症与3×WHD相似。
这项观察性研究未能证明转为4×WHD的患者有死亡率获益。要证明4×WHD的真正益处需要进行一项大型、设计良好的临床试验。我们的数据可能有助于此类研究的设计。