Sun Lova, Parikh Ravi B, Hubbard Rebecca A, Cashy John, Takvorian Samuel U, Vaughn David J, Robinson Kyle W, Narayan Vivek, Ky Bonnie
Division of Hematology/Oncology, Department of Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Abramson Cancer Center, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
JAMA Netw Open. 2021 Feb 1;4(2):e210070. doi: 10.1001/jamanetworkopen.2021.0070.
Cardiovascular disease is a leading cause of mortality in patients with prostate cancer, and androgen deprivation therapy (ADT) may worsen cardiovascular risk. Adherence to guideline-recommended assessment and management of cardiovascular risk factors (CVRFs) in patients initiating ADT is unknown.
To describe CVRF assessment and management in men with prostate cancer initiating ADT and overall.
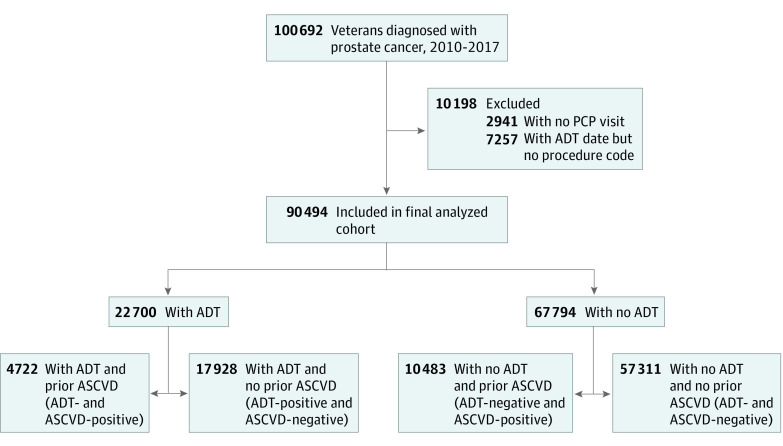
DESIGN, SETTING, AND PARTICIPANTS: A cross-sectional analysis of 90 494 men treated within the US Veterans Health Administration diagnosed with prostate cancer between January 1, 2010, and December 31, 2017, was conducted. Participants included men with a history of atherosclerotic cardiovascular disease (ASCVD), and treatment with ADT within 1 year of diagnosis. Data analysis was conducted from September 10, 2019, to July 1, 2020.
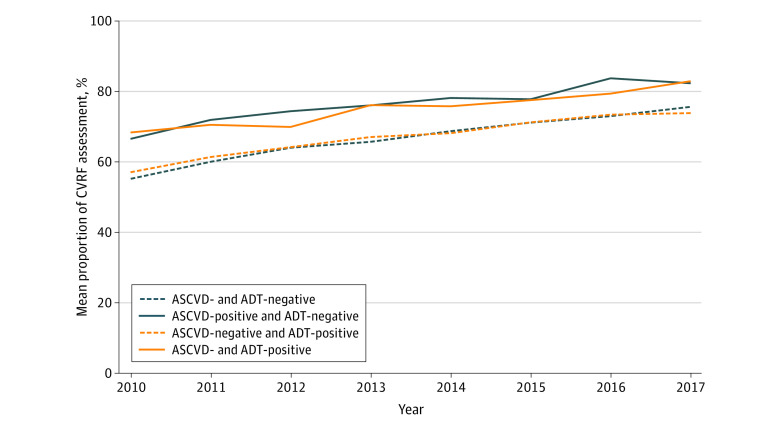
Rates of comprehensive CVRF assessment, uncontrolled CVRFs, and untreated CVRFs. Comprehensive CVRF assessment was defined as recorded measures for blood pressure, cholesterol, and glucose levels; CVRF control as blood pressure lower than 140/90 mm Hg, low-density lipoprotein cholesterol 130 mg/dL, and hemoglobin A1c less than 7%; and CVRF treatment as receipt of cardiac risk-reducing medications. Multivariable risk difference regression assessed the association between ASCVD and initiation of ADT and these outcomes.
Of 90 494 veterans, median age was 66 years (interquartile range, 62-70 years); and 22 700 men (25.1%) received ADT. Overall, 68.1% (95% CI, 67.8%-68.3%) of the men received comprehensive CVRF assessment; 54.1% (95% CI. 53.7%-54.4%) of those assessed had uncontrolled CVRFs, and 29.6% (95% CI, 29.2%-30.0%) of those with uncontrolled CVRFs were not receiving corresponding cardiac risk-reducing medication. Compared with the reference group of patients without ASCVD not receiving ADT, patients with ASCVD not receiving ADT had a 10.4% (95% CI, 9.5%-11.3%) higher probability of comprehensive CVRF assessment, 4.0% (95% CI, 2.9%-5.1%) lower risk of uncontrolled CVRFs, and 22.2% (95% CI, 21.1%-23.3%) lower risk of untreated CVRFs. Similar differences were observed in patients with ASCVD receiving ADT. In contrast, patients without ASCVD receiving ADT had only a 3.0% (95% CI, 2.1%-3.9%) higher probability of comprehensive CVRF assessment, 2.6% (95% CI, 1.6%-3.5%) higher risk of uncontrolled CVRFs, and 5.4% (95% CI, 4.2%-6.6%) lower risk of untreated CVRFs.
These findings suggest that veterans with prostate cancer had a high rate of underassessed and undertreated CVRFs, and ADT initiation was not associated with substantial improvements in CVRF assessment or management. These findings highlight gaps in care and the need for interventions to improve CVRF mitigation in this population.
心血管疾病是前列腺癌患者死亡的主要原因,雄激素剥夺疗法(ADT)可能会使心血管风险恶化。对于开始接受ADT治疗的患者,遵循指南推荐的心血管危险因素(CVRF)评估和管理情况尚不清楚。
描述开始接受ADT治疗的前列腺癌男性患者以及总体人群的CVRF评估和管理情况。
设计、背景和参与者:对2010年1月1日至2017年12月31日在美国退伍军人健康管理局接受治疗且被诊断为前列腺癌的90494名男性进行了横断面分析。参与者包括有动脉粥样硬化性心血管疾病(ASCVD)病史且在诊断后1年内接受ADT治疗的男性。数据分析于2019年9月10日至2020年7月1日进行。
全面CVRF评估率、未控制的CVRF率和未治疗的CVRF率。全面CVRF评估定义为记录血压、胆固醇和血糖水平的测量值;CVRF控制定义为血压低于140/90 mmHg、低密度脂蛋白胆固醇低于130 mg/dL以及糖化血红蛋白低于7%;CVRF治疗定义为接受降低心脏风险的药物治疗。多变量风险差异回归评估了ASCVD与开始ADT治疗以及这些结局之间的关联。
在90494名退伍军人中,中位年龄为66岁(四分位间距为62 - 70岁);22700名男性(25.1%)接受了ADT治疗。总体而言,68.1%(95%CI,67.8% - 68.3%)的男性接受了全面CVRF评估;在接受评估的患者中,54.1%(95%CI,53.7% - 54.4%)的CVRF未得到控制,在CVRF未得到控制的患者中,29.6%(95%CI,29.2% - 30.0%)未接受相应的降低心脏风险药物治疗。与未接受ADT治疗的无ASCVD患者参考组相比,未接受ADT治疗的ASCVD患者进行全面CVRF评估的概率高10.4%(95%CI,9.5% - 11.3%),CVRF未得到控制的风险低4.0%(95%CI,2.9% - 5.1%),未治疗的CVRF风险低22.2%(95%CI,21.1% - 23.3%)。在接受ADT治疗的ASCVD患者中也观察到了类似差异。相比之下,接受ADT治疗的无ASCVD患者进行全面CVRF评估的概率仅高3.0%(95%CI,2.1% - 3.9%),CVRF未得到控制的风险高2.6%(95%CI,1.6% - 3.5%),未治疗的CVRF风险低5.4%(95%CI,4.2% - 6.6%)。
这些发现表明,前列腺癌退伍军人中CVRF评估不足和治疗不足的发生率较高,开始ADT治疗与CVRF评估或管理的显著改善无关。这些发现凸显了护理方面的差距以及在该人群中改善CVRF缓解的干预措施的必要性。