Parsons I T, Stacey M J, Faconti L, Hill N, O'Hara J, Walter E, Farukh B, McNally R, Sharp H, Patten A, Grimaldi R, Gall N, Chowienczyk P, Woods D R
Research and Clinical Innovation, Royal Centre for Defence Medicine, Birmingham, England.
School of Cardiovascular Medicine and Sciences, King's College London, London, UK.
Eur J Appl Physiol. 2021 May;121(5):1451-1459. doi: 10.1007/s00421-021-04645-0. Epub 2021 Feb 24.
Heat stress exacerbates post-exercise hypotension (PEH) and cardiovascular disturbances from elevated body temperature may contribute to exertion-related incapacity. Mast cell degranulation and muscle mass are possible modifiers, though these hypotheses lack practical evidence. This study had three aims: (1) to characterise pre-post-responses in histamine and mast cell tryptase (MCT), (2) to investigate relationships between whole body muscle mass (WBMM) and changes in blood pressure post-marathon, (3) to identify any differences in incapacitated runners.
24 recreational runners were recruited and successfully completed the 2019 Brighton Marathon (COMPLETION). WBMM was measured at baseline. A further eight participants were recruited from incapacitated runners (COLLAPSE). Histamine, MCT, blood pressure, heart rate, body temperature and echocardiographic measures were taken before and after exercise (COMPLETION) and upon incapacitation (COLLAPSE).
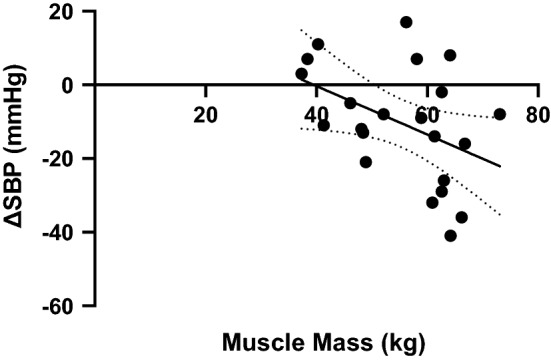
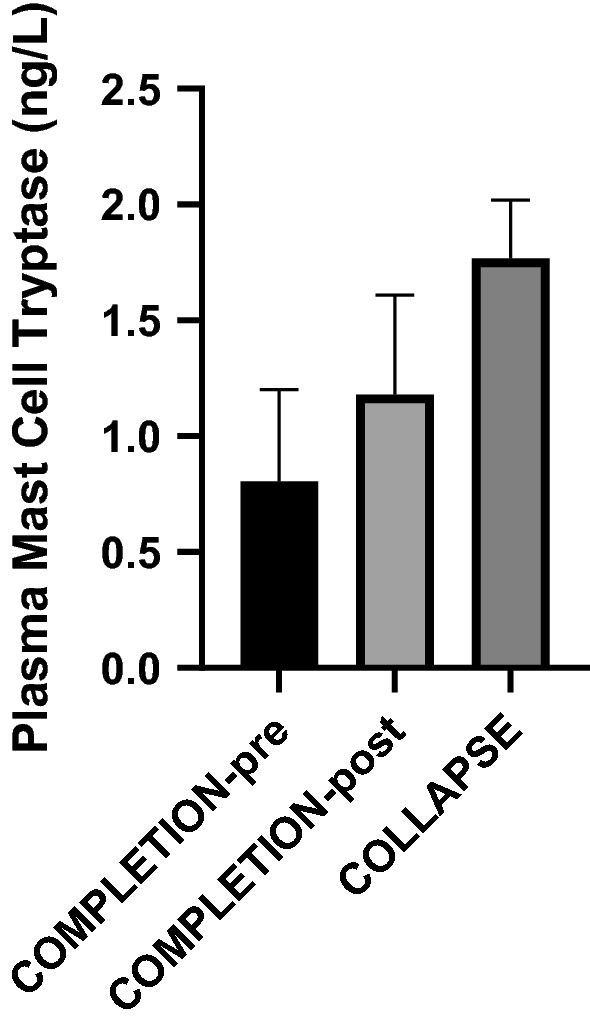
In completion, MCT increased by nearly 50% from baseline (p = 0.0049), whereas histamine and body temperature did not vary (p > 0.946). Systolic (SBP), diastolic (DBP) and mean (MAP) arterial blood pressures and systemic vascular resistance (SVR) declined (p < 0.019). WBMM negatively correlated with Δ SBP (r = - 0.43, p = 0.046). For collapse versus completion, there were significant elevations in MCT (1.77 ± 0.25 μg/L vs 1.18 ± 0.43 μg/L, p = 0.001) and body temperature (39.8 ± 1.3 °C vs 36.2 ± 0.8 °C, p < 0.0001) with a non-significant rise in histamine (9.6 ± 17.9 μg/L vs 13.7 ± 33.9 μg/L, p = 0.107) and significantly lower MAP, DBP and SVR (p < 0.033).
These data support the hypothesis that mast cell degranulation is a vasodilatory mechanism underlying PEH and exercise associated collapse. The magnitude of PEH is inversely proportional to the muscle mass and enhanced by concomitant body heating.
热应激会加剧运动后低血压(PEH),体温升高引起的心血管紊乱可能导致与运动相关的机能丧失。肥大细胞脱颗粒和肌肉量可能是影响因素,不过这些假设缺乏实际证据。本研究有三个目的:(1)描述组胺和肥大细胞类胰蛋白酶(MCT)在运动前后的变化,(2)研究全身肌肉量(WBMM)与马拉松赛后血压变化之间的关系,(3)确定失能跑步者之间的任何差异。
招募了24名业余跑步者,他们成功完成了2019年布莱顿马拉松赛(完赛组)。在基线时测量WBMM。从不明原因失能的跑步者中又招募了另外8名参与者(失能组)。在运动前和运动后(完赛组)以及失能时(失能组)测量组胺、MCT、血压、心率、体温和超声心动图指标。
在完赛组中,MCT较基线增加了近50%(p = 0.0049),而组胺和体温没有变化(p > 0.946)。收缩压(SBP)、舒张压(DBP)和平均动脉压(MAP)以及全身血管阻力(SVR)下降(p < 0.019)。WBMM与ΔSBP呈负相关(r = -0.43,p = 0.046)。与完赛组相比,失能组的MCT(1.77±0.25μg/L对1.18±0.43μg/L,p = 0.001)和体温(39.8±1.3°C对36.2±0.8°C)显著升高,组胺有不显著升高(9.6±17.9μg/L对13.7±33.9μg/L,p = 0.107),MAP、DBP和SVR显著降低(p < 0.033)。
这些数据支持以下假设,即肥大细胞脱颗粒是PEH和运动相关失能的一种血管舒张机制。PEH的程度与肌肉量成反比,并因同时存在的体温升高而增强。