de Montmollin Etienne, Schwebel Carole, Dupuis Claire, Garrouste-Orgeas Maité, da Silva Daniel, Azoulay Elie, Laurent Virginie, Thiéry Guillaume, Grinea Alexandra, Marcotte Guillaume, Oziel Johanna, Gainnier Marc, Siami Shidasp, Reignier Jean, Sztrymf Benjamin, Adrie Christophe, Ruckly Stephane, Sonneville Romain, Timsit Jean-François
Université de Paris, UMR 1137, IAME, Paris, France.
Assistance Publique - Hopitaux de Paris, Medical and Infectious Diseases ICU, Bichat-Claude Bernard Hospital, Paris, France.
Crit Care Explor. 2021 Feb 22;3(2):e0341. doi: 10.1097/CCE.0000000000000341. eCollection 2021 Feb.
The determinants of decisions to limit life support (withholding or withdrawal) in ventilated stroke patients have been evaluated mainly for patients with intracranial hemorrhages. We aimed to evaluate the frequency of life support limitations in ventilated ischemic and hemorrhagic stroke patients compared with a nonbrain-injured population and to determine factors associated with such decisions.
Multicenter prospective French observational study.
Fourteen ICUs of the French OutcomeRea network.
From 2005 to 2016, we included stroke patients and nonbrain-injured patients requiring invasive ventilation within 24 hours of ICU admission.
None.
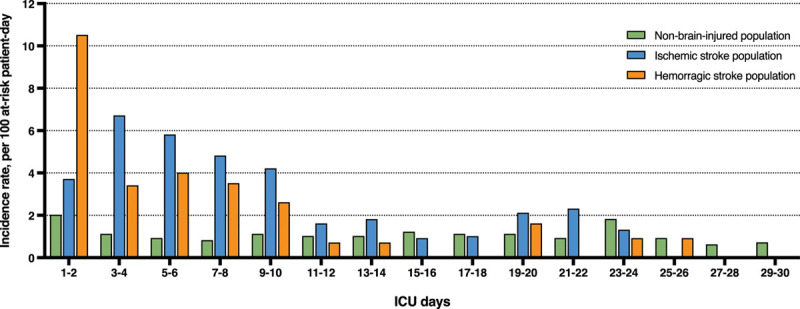
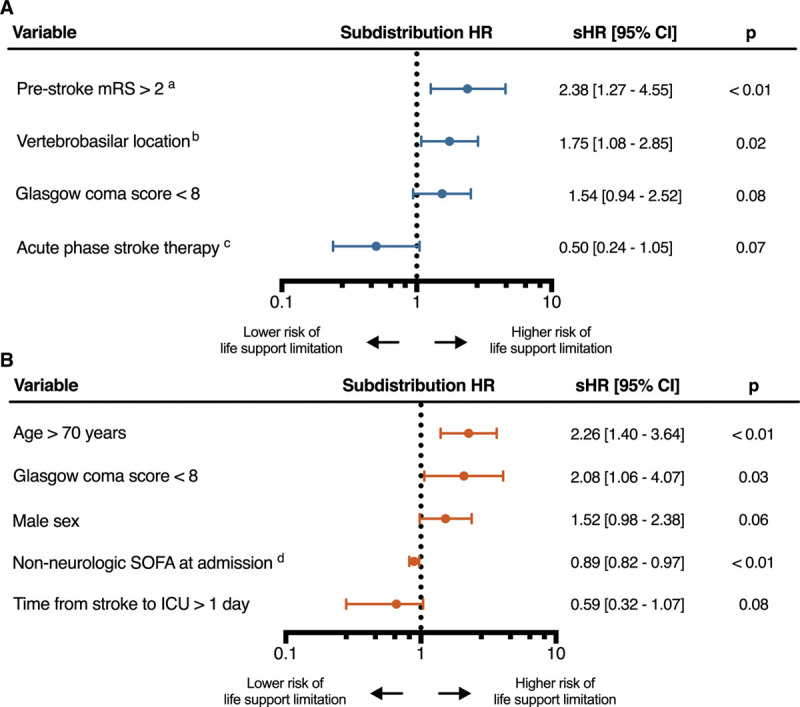
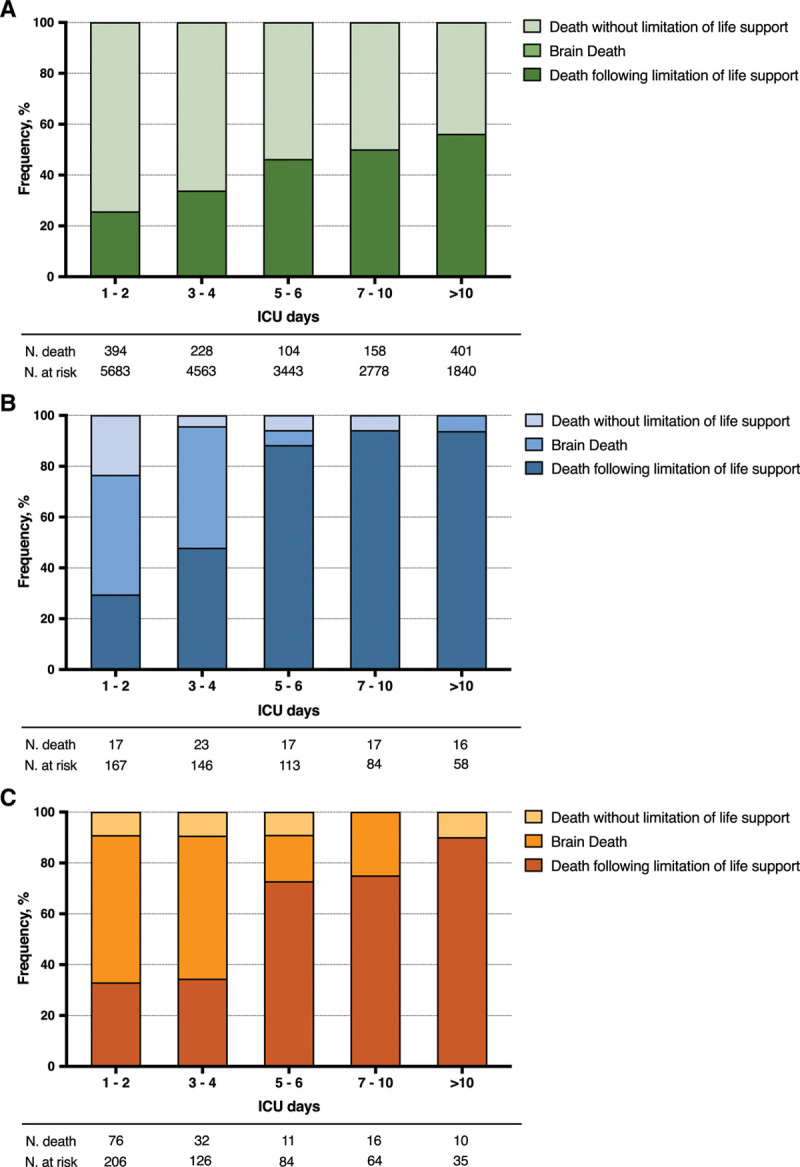
We identified 373 stroke patients (ischemic, = 167 [45%]; hemorrhagic, = 206 [55%]) and 5,683 nonbrain-injured patients. Decisions to limit life support were taken in 41% of ischemic stroke cases (vs nonbrain-injured patients, subdistribution hazard ratio, 3.59 [95% CI, 2.78-4.65]) and in 33% of hemorrhagic stroke cases (vs nonbrain-injured patients, subdistribution hazard ratio, 3.9 [95% CI, 2.97-5.11]). Time from ICU admission to the first limitation was longer in ischemic than in hemorrhagic stroke (5 [3-9] vs 2 d [1-6] d; < 0.01). Limitation of life support preceded ICU death in 70% of ischemic strokes and 45% of hemorrhagic strokes ( < 0.01). Life support limitations in ischemic stroke were increased by a vertebrobasilar location (vs anterior circulation, subdistribution hazard ratio, 1.61 [95% CI, 1.01-2.59]) and a prestroke modified Rankin score greater than 2 (2.38 [1.27-4.55]). In hemorrhagic stroke, an age greater than 70 years (2.29 [1.43-3.69]) and a Glasgow Coma Scale score less than 8 (2.15 [1.08-4.3]) were associated with an increased risk of limitation, whereas a higher nonneurologic admission Sequential Organ Failure Assessment score was associated with a reduced risk (per point, 0.89 [0.82-0.97]).
In ventilated stroke patients, decisions to limit life support are more than three times more frequent than in nonbrain-injured patients, with different timing and associated risk factors between ischemic and hemorrhagic strokes.
主要针对颅内出血患者评估了通气性卒中患者限制生命支持( withholding或withdrawal)决策的决定因素。我们旨在评估通气性缺血性和出血性卒中患者与非脑损伤人群相比生命支持受限的频率,并确定与这些决策相关的因素。
多中心前瞻性法国观察性研究。
法国OutcomeRea网络的14个重症监护病房。
2005年至2016年,我们纳入了在重症监护病房入院24小时内需要有创通气的卒中患者和非脑损伤患者。
无。
我们确定了373例卒中患者(缺血性,n = 167 [45%];出血性,n = 206 [55%])和5683例非脑损伤患者。41%的缺血性卒中病例做出了限制生命支持的决定(与非脑损伤患者相比,亚分布风险比,3.59 [95%CI,2.78 - 4.65]),33%的出血性卒中病例做出了限制生命支持的决定(与非脑损伤患者相比,亚分布风险比,3.9 [95%CI,2.97 - 5.11])。从重症监护病房入院到首次限制的时间,缺血性卒中比出血性卒中更长(5 [3 - 9]天对2 [1 - 6]天;P < 0.01)。70%的缺血性卒中和44出血性卒中在重症监护病房死亡前限制了生命支持(P < 0.01)。缺血性卒中生命支持受限因椎基底动脉部位(与前循环相比,亚分布风险比,1.61 [95%CI,1.01 - 2.59])和卒中前改良Rankin评分大于2(2.38 [1.27 - 4.55])而增加。在出血性卒中中,年龄大于70岁(2.29 [1.43 - 3.69])和格拉斯哥昏迷量表评分小于8(2.15 [1.08 - 4.3])与限制风险增加相关,而非神经科入院序贯器官衰竭评估评分较高与风险降低相关(每增加1分风险比为0.89 [0.82 - 0.97])。
在通气性卒中患者中,限制生命支持的决策比非脑损伤患者频繁三倍以上,缺血性和出血性卒中在时间和相关风险因素方面存在差异。