Pharmerit International, Berlin, Germany.
Pharmerit International, Rotterdam, Netherlands.
BMC Infect Dis. 2021 Feb 26;21(1):222. doi: 10.1186/s12879-021-05850-0.
The objective of this study was to assess the durability of response of dolutegravir (DTG) as an antiretroviral core agent by comparing its efficacy and safety with other recommended or commonly used core agents up to 96-weeks (W96).
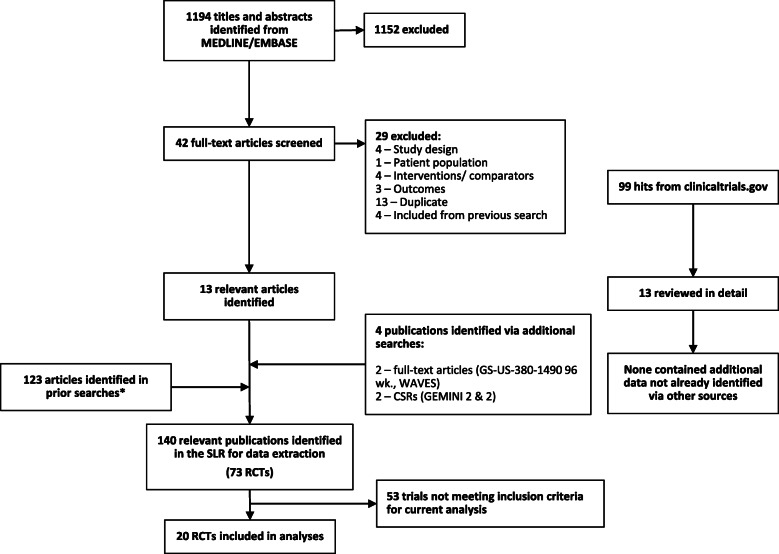
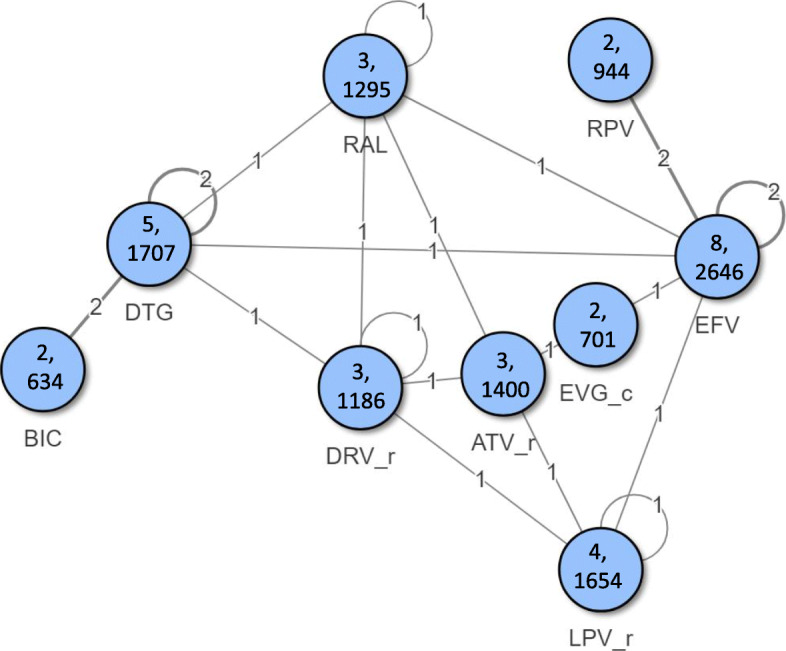
A previously published systematic review was updated to identify phase 3/4 randomised controlled trials (RCTs) of core agents in treatment-naïve HIV-1 patients. Efficacy [virologic suppression (VS), CD4 cell change from baseline] and safety [adverse events [AEs], discontinuations, drug-related AEs [DRAEs]] were analysed at W96 using Bayesian network meta-analysis (NMA) adjusting for nucleoside/nucleotide reverse transcriptase inhibitors' (NRTIs') backbone. Subgroups of patients with VL > 100,000 copies/mL or CD4 ≤ 200 cells/μL at baseline were analysed separately.
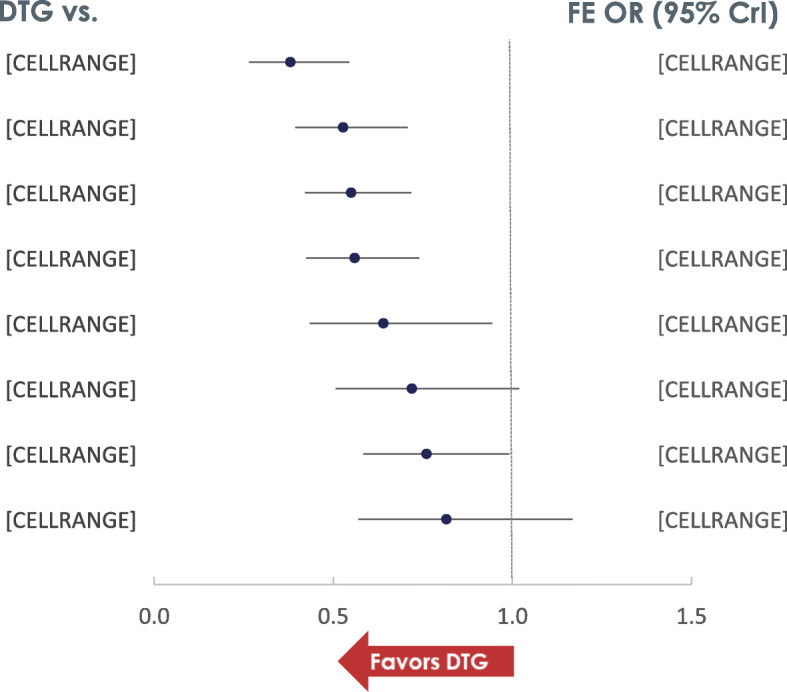
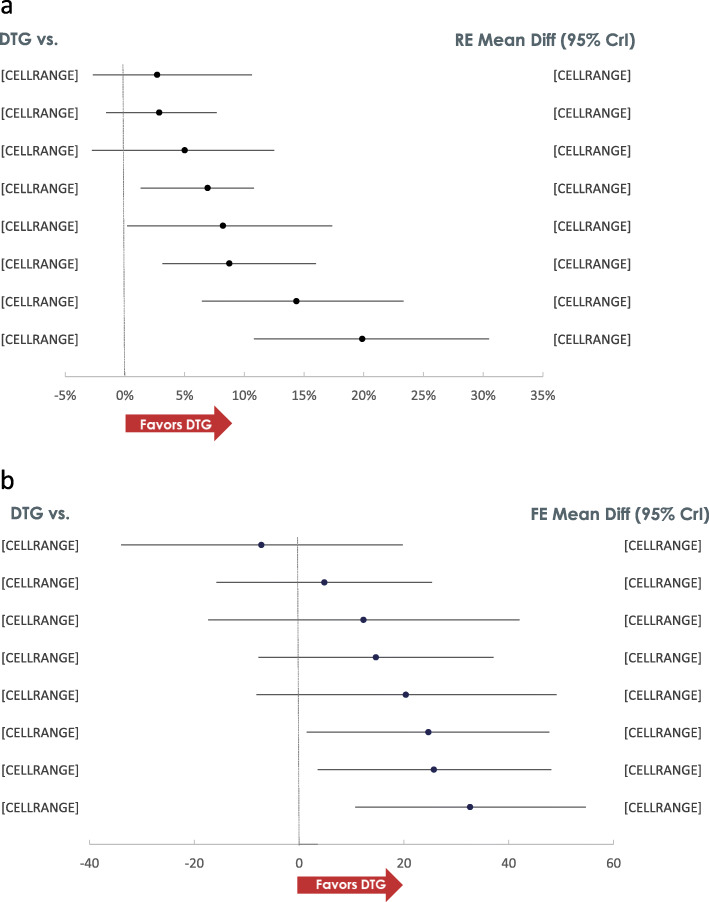
The NMA included 20 studies reporting data at W96. A higher proportion of patients receiving DTG achieved VS compared to those on protease inhibitors [PI:Range:8.7%(CrI:3.1,16.0)-19.9%(10.8,30.5)], efavirenz [EFV:6.9%(1.3,10.8)] and cobicistat-boosted elvitegravir [EVG/c:8.2%(0.2,17.4)], and similar but numerically higher compared to rilpivirine [RPV:5.0%(- 2.8,12.5)], raltegravir [RAL:2.9%(- 1.6,7.7)] and bictegravir [BIC:2.7%(- 2.7,10.6)]. The probability that more patients on DTG would achieve VS at W96 compared to any other core agent was greater than 80%. A higher proportion of patients on DTG achieved VS compared to PI/rs [Range:33.1%(13.6,50.4)-45.3%(24.1,61.6)] and RAL [16.7%(3.3,31.2)] in patients with VL > 100,000 copies/mL at baseline, and similar VS was achieved in patients with CD4 ≤ 200 cells/μL at baseline. DTG also achieved greater increase in CD4 cells from baseline compared to EFV [32.6(10.7,54.7)], ritonavir-boosted darunavir [DRV/r:25.7(3.6,48.1)] and BIC [24.7(1.5,47.7)]. Patients receiving DTG had lower odds of discontinuing therapy by W96 compared to PI/rs, EFV, RAL and EVG/c. Patients on DTG had lower odds of experiencing an adverse event (AE) compared to patients on EFV [odds ratio:0.6(0.3,0.9)], ATV/r [0.4(0.3,0.6)] and LPV/r [0.3(0.2,0.5)]. For patients on DTG, the odds of experiencing a drug-related AE were lower than the odds for patients on EFV [0.3(0.2,0.4)], comparable to patients on RAL [1.1(0.8,1.4)] and higher than those on BIC [1.5(1.1,2.0)].
Un-boosted integrase inhibitors had better efficacy and similar safety compared to PI/rs at W96 in treatment-naïve patients with HIV-1, with DTG being among the most efficacious core agent, particularly in patients with baseline VL > 100,000 copies/mL or ≤ 200 CD4 cells/μL, who can be difficult to treat.
本研究旨在通过比较多替拉韦(DTG)作为抗逆转录病毒核心药物的疗效和安全性,评估其在 96 周(W96)时的反应持久性,其他推荐或常用的核心药物。
对之前发表的系统评价进行了更新,以确定治疗初治 HIV-1 患者的核心药物的 3/4 期随机对照试验(RCT)。使用贝叶斯网络荟萃分析(NMA)调整核苷/核苷酸逆转录酶抑制剂(NRTIs)的主干,在 W96 时分析疗效[病毒学抑制(VS),CD4 细胞从基线变化]和安全性[不良事件(AE),停药,药物相关 AE(DRAEs)]。单独分析基线 VL>100,000 拷贝/mL 或 CD4≤200 个/μL 的患者的亚组。
NMA 包括 20 项报告 W96 数据的研究。与蛋白酶抑制剂(PI)相比,接受 DTG 的患者中达到 VS 的比例更高[PI:范围:8.7%(CrI:3.1,16.0)-19.9%(10.8,30.5)],依非韦伦[EFV:6.9%(1.3,10.8)]和考比司他增强型艾维雷韦[EVG/c:8.2%(0.2,17.4)],与 rilpivirine[RPV:5.0%(-2.8,12.5)]、raltegravir[RAL:2.9%(-1.6,7.7)]和 bictegravir[BIC:2.7%(-2.7,10.6)]相似,但数值更高。与任何其他核心药物相比,接受 DTG 的患者达到 VS 的可能性大于 80%。与 PI/rs 相比,接受 DTG 的患者达到 VS 的比例更高[范围:33.1%(13.6,50.4)-45.3%(24.1,61.6)]和 RAL[16.7%(3.3,31.2)],在基线 VL>100,000 拷贝/mL 的患者中,与基线 CD4≤200 个/μL 的患者相比,达到了相似的 VS。DTG 也实现了比 EFV[32.6(10.7,54.7)]、ritonavir 增强型达鲁那韦[DRV/r:25.7(3.6,48.1)]和 BIC[24.7(1.5,47.7)]更大的 CD4 细胞从基线增加。与 PI/rs、EFV、RAL 和 EVG/c 相比,接受 DTG 的患者在 W96 时停药的可能性较低。与 EFV[比值比:0.6(0.3,0.9)]、ATV/r[0.4(0.3,0.6)]和 LPV/r[0.3(0.2,0.5)]相比,接受 DTG 的患者发生不良事件(AE)的可能性较低。对于接受 DTG 的患者,药物相关 AE 的可能性低于 EFV 患者[比值比:0.3(0.2,0.4)],与 RAL 患者[1.1(0.8,1.4)]相似,高于 BIC 患者[1.5(1.1,2.0)]。
在治疗初治 HIV-1 患者中,未增强的整合酶抑制剂在 W96 时的疗效优于 PI/rs,安全性相似,其中 DTG 是最有效的核心药物之一,特别是在基线 VL>100,000 拷贝/mL 或 CD4≤200 个/μL 的患者中,这些患者的治疗难度较大。