Moriyama Shohei, Fukata Mitsuhiro, Tatsumoto Ryoma, Kono Mihoko
Department of Hematology, Oncology and Cardiovascular Medicine, Kyushu University Hospital, Maidashi 3-1-1, Higashi-ku, Fukuoka 812-8582, Japan.
Department of Onco-Cardiology, National Hospital Organization Kyushu Cancer Center, Fukuoka 811-1395, Japan.
Eur Heart J Case Rep. 2021 Feb 1;5(1):ytab002. doi: 10.1093/ehjcr/ytab002. eCollection 2021 Jan.
Immune checkpoint inhibitors (ICIs) can cause cardiac immune-related adverse events (irAEs), including pericarditis. Cardiovascular events related to pericardial irAE are less frequent, but fulminant forms can be fatal. However, the diagnosis and treatment strategies for pericardial irAE have not established.
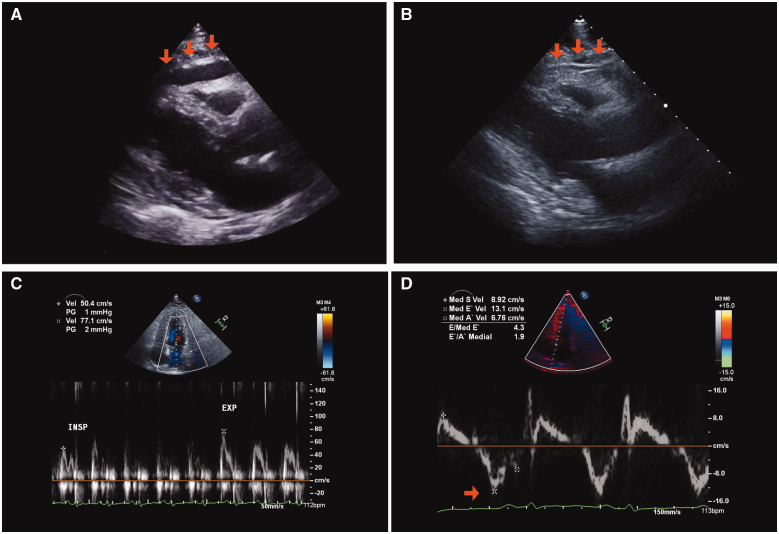
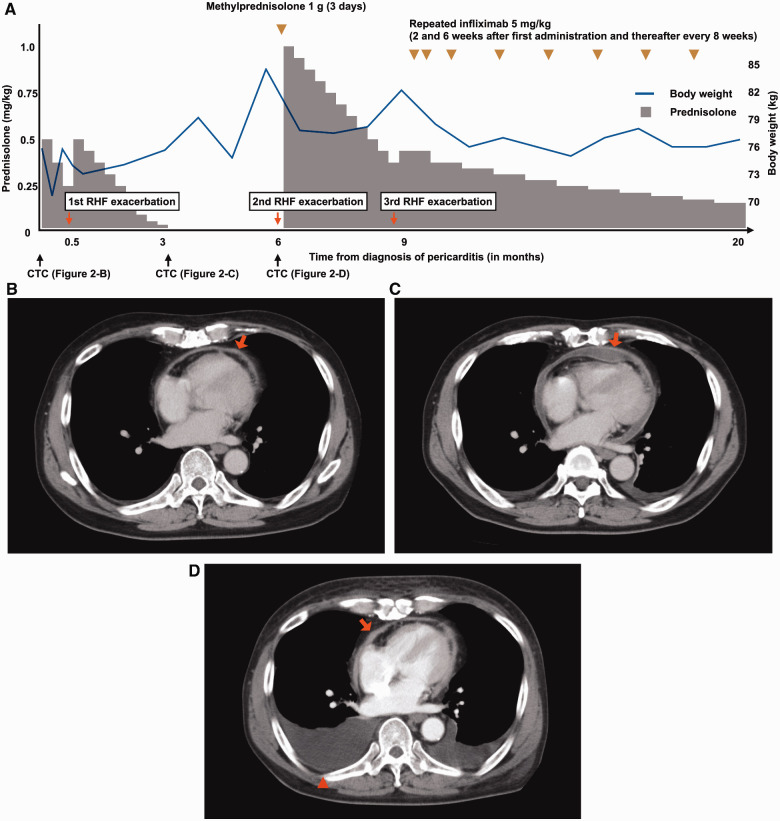
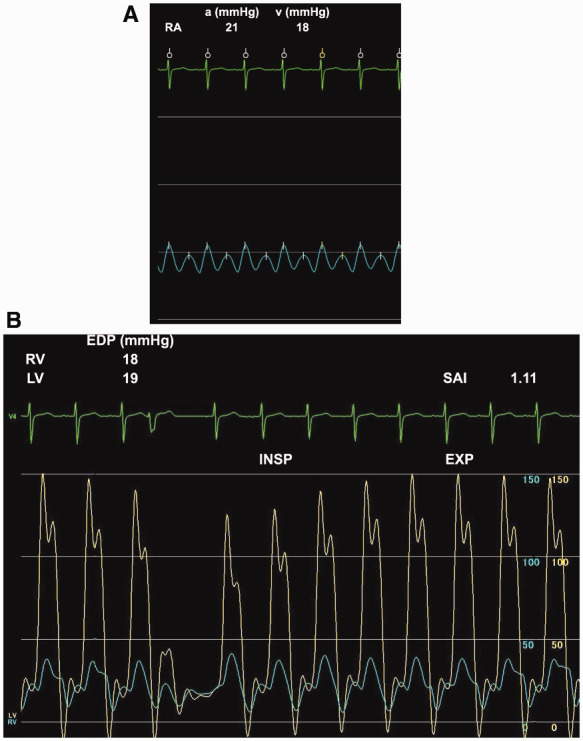
A 58-year-old man was diagnosed with advanced non-small-cell lung cancer and nivolumab was administered as 5th-line therapy. Eighteen months after the initiation of nivolumab, the patient developed limb oedema and increased body weight. Although a favourable response of the cancer was observed, pericardial thickening and effusion were newly detected. He was diagnosed with irAE pericarditis after excluding other causes of pericarditis. Nivolumab was suspended and a high-dose corticosteroid was initiated. However, right heart failure (RHF) symptoms were exacerbated during the tapering of corticosteroid because acute pericarditis developed to steroid-refractory constrictive pericarditis. To suppress sustained inflammation of the pericardium, infliximab, a tumour necrosis factor-alfa inhibitor, was initiated. After the initiation of infliximab, the corticosteroid dose was tapered without deterioration of RHF. Exacerbation of lung cancer by irAE treatment including infliximab was not observed.
IrAE should be considered when pericarditis develops after the administration of ICI even after a long period from its initiation. Infliximab rescue therapy may be considered as a 2nd-line therapy for steroid-refractory irAE pericarditis even with constrictive physiology.
免疫检查点抑制剂(ICI)可引起心脏免疫相关不良事件(irAE),包括心包炎。与心包irAE相关的心血管事件较少见,但暴发性形式可能致命。然而,心包irAE的诊断和治疗策略尚未确立。
一名58岁男性被诊断为晚期非小细胞肺癌,接受纳武单抗作为五线治疗。纳武单抗开始使用18个月后,患者出现肢体水肿和体重增加。尽管观察到癌症有良好反应,但新检测到心包增厚和积液。排除其他心包炎病因后,他被诊断为irAE心包炎。纳武单抗暂停使用,并开始使用高剂量皮质类固醇。然而,在皮质类固醇减量过程中,右心衰竭(RHF)症状加重,因为急性心包炎发展为类固醇难治性缩窄性心包炎。为抑制心包的持续炎症,开始使用肿瘤坏死因子-α抑制剂英夫利昔单抗。开始使用英夫利昔单抗后,皮质类固醇剂量逐渐减少,RHF未恶化。未观察到包括英夫利昔单抗在内的irAE治疗导致肺癌恶化。
即使在ICI给药后很长时间出现心包炎,也应考虑irAE。即使存在缩窄性生理状况,英夫利昔单抗挽救治疗也可作为类固醇难治性irAE心包炎的二线治疗。