Karkhanis Reena, Wijeysundera Harindra C, Tam Derrick Y, Oh Paul, Alter David A, Yu Bing, Kiss Alex, Fremes Stephen E
Division of Cardiac Surgery, Schulich Heart Centre, Department of Surgery, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada.
Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada.
CJC Open. 2020 Oct 12;3(2):167-175. doi: 10.1016/j.cjco.2020.10.004. eCollection 2021 Feb.
Although cardiac rehabilitation (CR) has proven to have short- and mid-term benefit in treatment of coronary artery disease, its long-term benefit in patients who have undergone coronary artery bypass grafting (CABG) is less certain. Our objective was to examine the late outcomes of patients who attended CR within the first year after CABG.
Adult CABG patients referred to Toronto Rehabilitation Institute (CR group: were referred and attended at least 1 session; No-CR group: were referred but did not attend) between January 1996 and September 2008 were identified through linkages with clinical and provincial administrative databases for comorbidities and outcome ascertainment. The primary outcome was a composite of all-cause mortality, acute myocardial infarction, stroke or repeat revascularization (major adverse cardiac and cerebrovascular events [MACCE]). The secondary outcome was all-cause mortality. Multivariable Cox proportional hazard models were used to assess the CR treatment effect, adjusting for baseline characteristics.
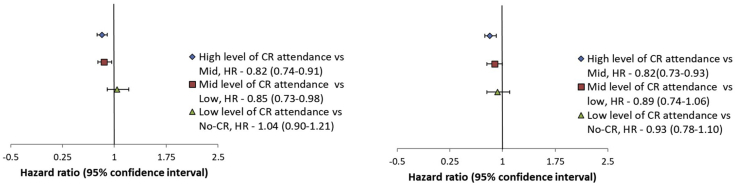
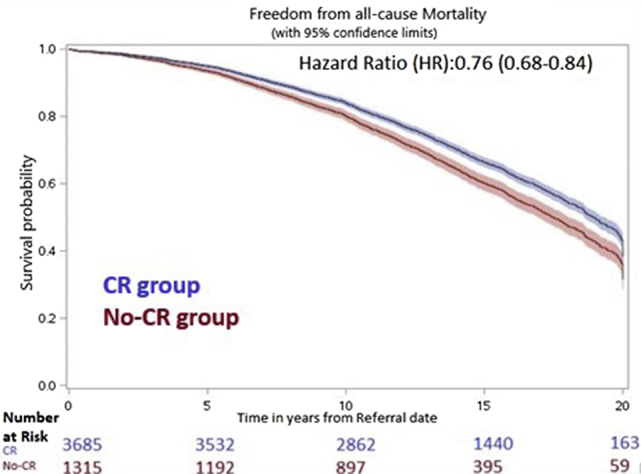
The study cohort consisted of 5,000 patients-3,685 (73.7%) in the CR group and 1,315 (26.3%) in the No-CR group. Median referral time was 32.5 days, and follow-up was 13.1 years. The CR group patients, compared with the No-CR group, were younger (age 62.6 ± 9.6 vs 64.0 ± 10.5 years), were more likely to be male (85.0% vs 79.5%), and had fewer cardiac comorbidities. In adjusted analyses, the CR group was associated with decreased MACCE (hazard ratio 0.83, 95% confidence interval 0.75-0.91, < 0.0001) and a higher adjusted survival at 15 years (66.3% vs 60.1%, hazard ratio 0.76, 95% confidence interval 0.68-0.84, < 0.0001), as compared with the No-CR group.
There was a reduction in MACCE and late mortality associated with CR attendance, highlighting the importance of patient referral and participation in CR after CABG.
尽管心脏康复(CR)已被证明在治疗冠状动脉疾病方面具有短期和中期益处,但其对接受冠状动脉旁路移植术(CABG)患者的长期益处尚不确定。我们的目的是研究CABG术后第一年内参加CR的患者的晚期结局。
通过与临床和省级行政数据库建立联系,以确定合并症和结局,识别1996年1月至2008年9月期间转诊至多伦多康复研究所的成年CABG患者(CR组:被转诊并至少参加了1次治疗;非CR组:被转诊但未参加)。主要结局是全因死亡率、急性心肌梗死、中风或再次血运重建(主要不良心脏和脑血管事件[MACCE])的综合指标。次要结局是全因死亡率。使用多变量Cox比例风险模型评估CR治疗效果,并对基线特征进行调整。
研究队列包括5000名患者,CR组3685名(73.7%),非CR组1315名(26.3%)。中位转诊时间为32.5天,随访时间为13.1年。与非CR组相比,CR组患者更年轻(年龄62.6±9.6岁对64.0±10.5岁),男性比例更高(85.0%对79.5%),心脏合并症更少。在调整分析中,与非CR组相比,CR组与MACCE降低相关(风险比0.83,95%置信区间0.75 - 0.91,P<0.0001),15年时调整后的生存率更高(66.3%对60.1%,风险比0.76,95%置信区间0.68 - 0.84,P<0.0001)。
参加CR与MACCE降低和晚期死亡率降低相关,突出了CABG术后患者转诊和参与CR的重要性。