Division of Allergy, Immunology and Rheumatology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan.
Division of Allergy, Immunology and Rheumatology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Clin Rheumatol. 2021 Sep;40(9):3755-3763. doi: 10.1007/s10067-021-05660-4. Epub 2021 Mar 1.
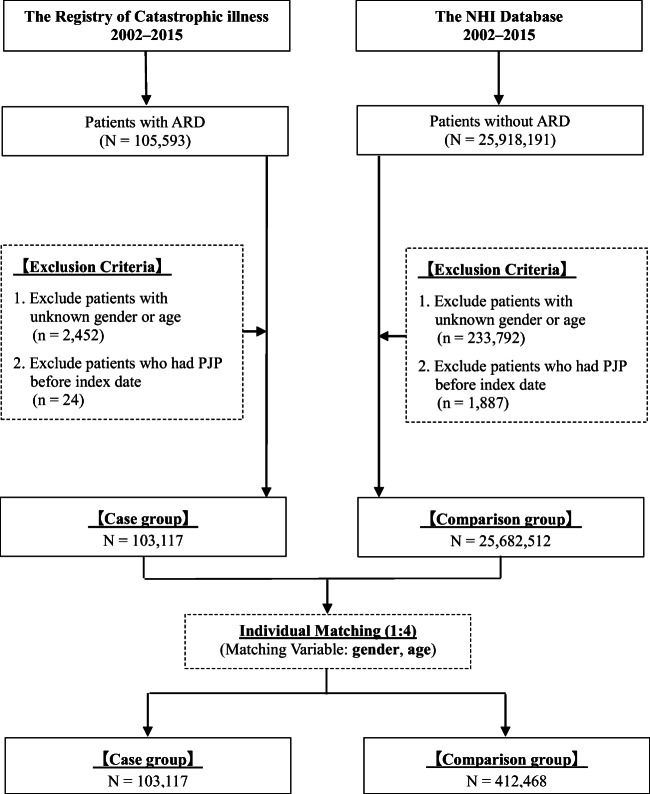
To compare Pneumocystis jirovecii pneumonia (PJP) risk between patients with autoimmune rheumatic diseases (ARD) and the general population METHODS: We identified patients with ARD recorded in the National Health Insurance Research Database of Taiwan from 2002 to 2015 and randomly selected a comparison cohort from the general population matched for age and sex. We analyzed PJP risk stratified by sex, age, comorbidities, and medications using Cox proportional hazard model.
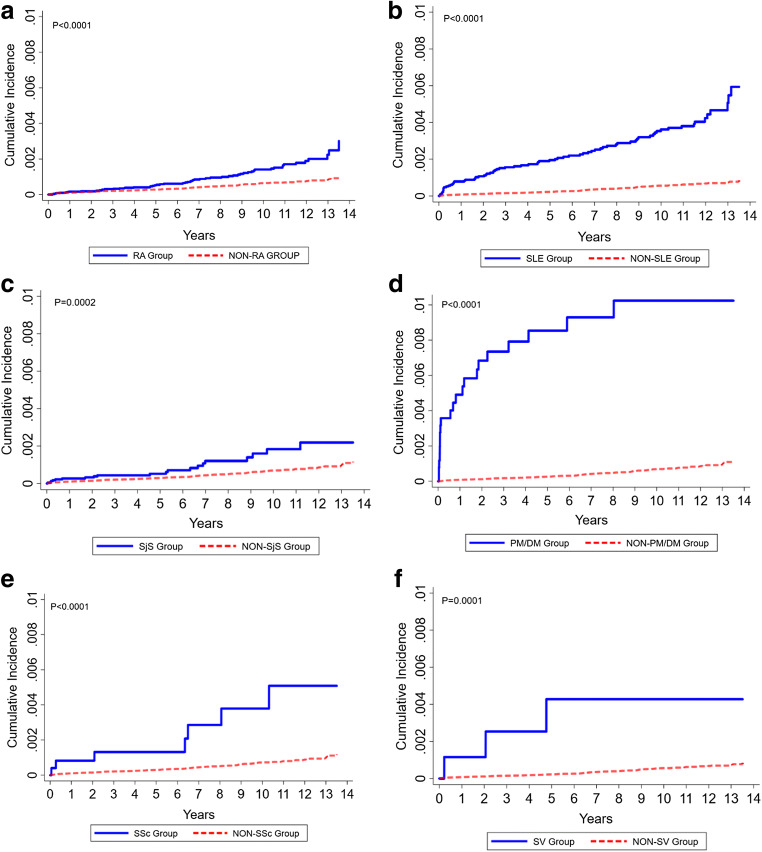
We enrolled 103,117 patients with ARD. PJP risk significantly increased in patients with any ARD and with each individual ARD like rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), Sjogren's syndrome (SjS), polymyositis and dermatomyositis (PM/DM), systemic sclerosis (SSc), and systemic vasculitis. Patients with PM/DM showed prominent risk with incidence rate of 12.47/100,000 patient year (95% confidence interval (CI), 32.16-86.70). In a time-dependent Cox proportional hazard model with comorbidities and medications as covariates, PM/DM, SSc, SLE, and SjS significantly increased adjusted hazard ratios (aHR) of 5.40, 5.12, 4.09, and 3.64, respectively (95% CI of 2.82-10.35, 2.16-12.13, 2.41-6.95, and 2.06-6.42, respectively). AHR after adjusting for male sex, cancer, human immunodeficiency virus infection (HIV), and interstitial lung disease also significantly increased. Use of daily oral steroid dose of >10 mg conferred the highest risk followed by mycophenolate. Use of injected steroids, cyclophosphamide, biological agents, methotrexate, and cyclosporine conferred a significantly higher risk.
Underlying ARD significantly predisposes patients to PJP, with PM/DM posing the highest threat. In addition to underlying disease, comorbidities and concomitant immunosuppressants are major risks. The strongest risk is recent daily steroid dose of >10 mg. Mycophenolate seems to be a more prominent risk factor than cyclophosphamide. Key Points • Autoimmune rheumatic diseases (ARD) significantly increased the overall risk of PJP, and so did each individual ARD. • Use of steroids, mycophenolate, cyclophosphamide, biological agents, methotrexate, and cyclosporine all significantly increased risk of PJP. • Male, elderly, malignancy, HIV, and interstitial lung disease are also related to increased risk of PJP. • Underlying ARD, comorbidities, and use of immunosuppressant should all be considered in determining the overall risk of PJP.
比较患有自身免疫性风湿病(ARD)与普通人群的卡氏肺孢子菌肺炎(PJP)风险。
我们从台湾全民健康保险研究数据库中确定了 2002 年至 2015 年记录的 ARD 患者,并按年龄和性别随机选择了普通人群的对照队列。我们使用 Cox 比例风险模型,按性别、年龄、合并症和药物分层分析 PJP 风险。
我们纳入了 103117 名 ARD 患者。任何 ARD 患者和患有特定 ARD 的患者(如类风湿关节炎、系统性红斑狼疮、干燥综合征、多发性肌炎和皮肌炎、系统性硬皮病和系统性血管炎)的 PJP 风险显著增加。多发性肌炎和皮肌炎患者的风险最为显著,发病率为 12.47/100000 患者年(95%置信区间为 32.16-86.70)。在纳入合并症和药物作为协变量的时间依赖性 Cox 比例风险模型中,多发性肌炎和皮肌炎、系统性硬皮病、系统性红斑狼疮和干燥综合征显著增加了调整后的危险比(aHR)分别为 5.40、5.12、4.09 和 3.64(95%CI 分别为 2.82-10.35、2.16-12.13、2.41-6.95 和 2.06-6.42)。调整男性、癌症、人类免疫缺陷病毒感染(HIV)和间质性肺病后,aHR 也显著增加。每日口服皮质类固醇剂量>10mg 导致的风险最高,其次是霉酚酸酯。使用注射用皮质类固醇、环磷酰胺、生物制剂、甲氨蝶呤和环孢素会导致更高的风险。
潜在的 ARD 显著增加了患者患 PJP 的风险,多发性肌炎和皮肌炎的风险最高。除了基础疾病外,合并症和同时使用的免疫抑制剂也是主要风险。最近每日>10mg 的皮质类固醇剂量风险最大。霉酚酸酯似乎比环磷酰胺更显著的风险因素。
自身免疫性风湿病(ARD)显著增加了 PJP 的总体风险,而每一种 ARD 也是如此。
皮质类固醇、霉酚酸酯、环磷酰胺、生物制剂、甲氨蝶呤和环孢素的使用均显著增加了 PJP 的风险。
男性、老年、恶性肿瘤、HIV 和间质性肺病也与 PJP 风险增加有关。
在确定 PJP 的总体风险时,应考虑潜在的 ARD、合并症和免疫抑制剂的使用。