Green Lane Cardiovascular Service, Auckland City Hospital, Private Bag 92024, Auckland 1030, New Zealand
Department of Medicine, University of Auckland, New Zealand.
BMJ. 2021 Mar 2;372:n355. doi: 10.1136/bmj.n355.
To determine the association between high flow supplementary oxygen and 30 day mortality in patients presenting with a suspected acute coronary syndrome (ACS).
Pragmatic, cluster randomised, crossover trial.
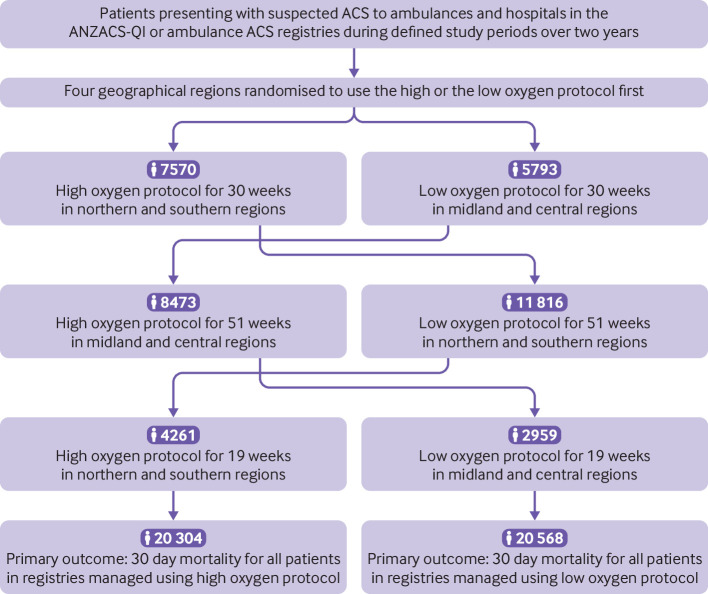
Four geographical regions in New Zealand.
40 872 patients with suspected or confirmed ACS included in the All New Zealand Acute Coronary Syndrome Quality Improvement registry or ambulance ACS pathway during the study periods. 20 304 patients were managed using the high oxygen protocol and 20 568 were managed using the low oxygen protocol. Final diagnosis of ST elevation myocardial infarction (STEMI) and non-STEMI were determined from the registry and ICD-10 discharge codes.
The four geographical regions were randomly allocated to each of two oxygen protocols in six month blocks over two years. The high oxygen protocol recommended oxygen at 6-8 L/min by face mask for ischaemic symptoms or electrocardiographic changes, irrespective of the transcapillary oxygen saturation (SpO). The low oxygen protocol recommended oxygen only if SpO was less than 90%, with a target SpO of less than 95%.
30 day all cause mortality determined from linkage to administrative data.
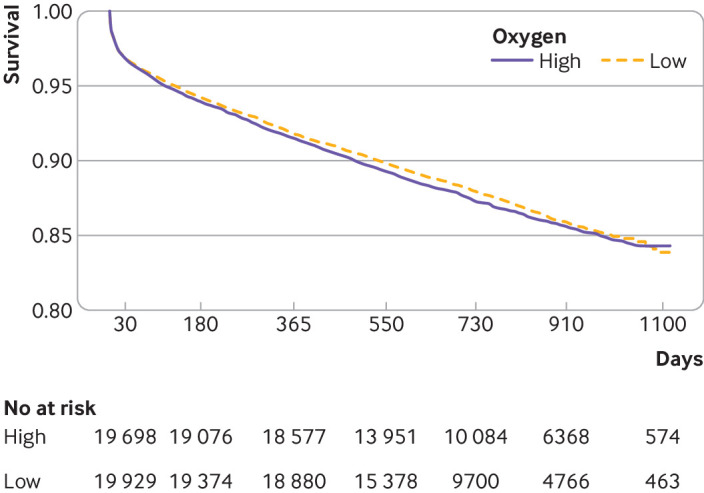
Personal and clinical characteristics of patients managed under both oxygen protocols were well matched. For patients with suspected ACS, 30 day mortality for the high and low oxygen groups was 613 (3.0%) and 642 (3.1%), respectively (odds ratio 0.97, 95% confidence interval 0.86 to 1.08). For 4159 (10%) patients with STEMI, 30 day mortality for the high and low oxygen groups was 8.8% (n=178) and 10.6% (n=225), respectively (0.81, 0.66 to 1.00) and for 10 218 (25%) patients with non-STEMI was 3.6% (n=187) and 3.5% (n=176), respectively (1.05, 0.85 to 1.29).
In a large patient cohort presenting with suspected ACS, high flow oxygen was not associated with an increase or decrease in 30 day mortality.
ANZ Clinical Trials ACTRN12616000461493.
确定在疑似急性冠状动脉综合征(ACS)患者中,高流量补充氧气与 30 天死亡率之间的关联。
实用、集群随机、交叉试验。
新西兰的四个地理区域。
在研究期间,纳入了全新西兰急性冠状动脉综合征质量改进登记处或救护车 ACS 途径的疑似或确诊 ACS 的 40872 名患者。20304 名患者接受高氧方案治疗,20568 名患者接受低氧方案治疗。ST 段抬高型心肌梗死(STEMI)和非 ST 段抬高型心肌梗死的最终诊断来自登记处和 ICD-10 出院代码。
在两年内,将四个地理区域随机分配到两个氧气方案中的每一个,每个方案持续六个月。高氧方案建议对缺血症状或心电图改变的患者通过面罩提供 6-8 L/min 的氧气,而不考虑毛细血管氧饱和度(SpO2)。低氧方案仅在 SpO2 低于 90%时建议吸氧,目标 SpO2 低于 95%。
通过与行政数据的链接确定 30 天全因死亡率。
接受两种氧气方案治疗的患者的个人和临床特征均匹配良好。对于疑似 ACS 的患者,高氧组和低氧组的 30 天死亡率分别为 613(3.0%)和 642(3.1%)(比值比 0.97,95%置信区间 0.86 至 1.08)。对于 4159 名(10%)STEMI 患者,高氧组和低氧组的 30 天死亡率分别为 8.8%(n=178)和 10.6%(n=225)(0.81,0.66 至 1.00),对于 10218 名(25%)非 STEMI 患者,30 天死亡率分别为 3.6%(n=187)和 3.5%(n=176)(1.05,0.85 至 1.29)。
在一个有大量疑似 ACS 患者的队列中,高流量氧气与 30 天死亡率的增加或降低无关。
ANZ 临床试验 ACTRN12616000461493。