Chiang Chi-Leung, Chan Sik-Kwan, Lee Shing-Fung, Choi Horace Cheuk-Wai
Department of Clinical Oncology, University of Hong Kong, Hong Kong.
Department of Clinical Oncology, Tuen Mun Hospital, Hong Kong.
Cancers (Basel). 2021 Feb 24;13(5):931. doi: 10.3390/cancers13050931.
The IMbrave 150 trial revealed that atezolizumab plus bevacizumab (atezo-bev) improves survival in patients with unresectable hepatocellular carcinoma (HCC) (1 year survival rate: 67.2% vs. 54.6%). We assessed the cost-effectiveness of atezo-bev vs. sorafenib as first-line therapy in patients with unresectable HCC from the US payer perspective.
Using data from the IMbrave 150, we developed a Markov model to compare the lifetime cost and efficacy of atezo-bev as first-line systemic therapy in HCC with those of sorafenib. The main outcomes were life-years, quality-adjusted life-years (QALYs), lifetime costs, and incremental cost-effectiveness ratio (ICER).
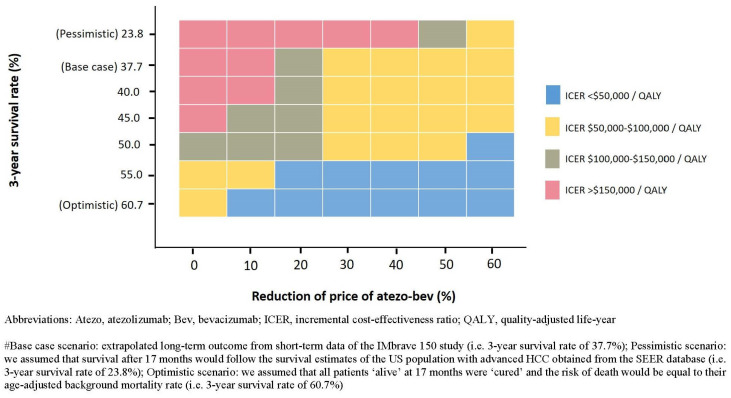
Atezo-bev demonstrated a gain of 0.44 QALYs, with an additional cost of USD 79,074. The ICER of atezo-bev was USD 179,729 per QALY when compared with sorafenib. The model was most sensitive to the overall survival hazard ratio and body weight. If we assumed that all patients at the end of the IMbrave 150 trial were cured of HCC, atezo-bev was cost-effective (ICER USD 53,854 per QALY). However, if all patients followed the Surveillance, Epidemiology, and End Results data, the ICER of atezo-bev was USD 385,857 per QALY. Reducing the price of atezo-bev by 20% and 29% would satisfy the USD 150,000/QALY and 100,000/QALY willingness-to-pay threshold. Moreover, capping the duration of therapy to ≤12 months or reducing the dosage of bev to ≤10 mg/kg would render atezo-bev cost-effective.
The long-term effectiveness of atezo-bev is a critical but uncertain determinant of its cost-effectiveness. Price reduction would favorably influence cost-effectiveness, even if long-term clinical outcomes were modest. Further studies to optimize the duration and dosage of therapy are warranted.
IMbrave 150试验显示,阿替利珠单抗联合贝伐珠单抗(阿替利珠单抗-贝伐珠单抗)可提高不可切除肝细胞癌(HCC)患者的生存率(1年生存率:67.2%对54.6%)。我们从美国医保支付方的角度评估了阿替利珠单抗-贝伐珠单抗与索拉非尼作为不可切除HCC患者一线治疗的成本效益。
利用IMbrave 150的数据,我们建立了一个马尔可夫模型,以比较阿替利珠单抗-贝伐珠单抗作为HCC一线全身治疗与索拉非尼的终身成本和疗效。主要结局指标为生命年、质量调整生命年(QALY)、终身成本和增量成本效益比(ICER)。
阿替利珠单抗-贝伐珠单抗显示获得了0.44个QALY,但额外成本为79,074美元。与索拉非尼相比,阿替利珠单抗-贝伐珠单抗的ICER为每QALY 179,729美元。该模型对总生存风险比和体重最为敏感。如果我们假设IMbrave 150试验结束时所有患者的HCC均已治愈,那么阿替利珠单抗-贝伐珠单抗具有成本效益(ICER为每QALY 53,854美元)。然而,如果所有患者遵循监测、流行病学和最终结果数据,阿替利珠单抗-贝伐珠单抗的ICER为每QALY 385,857美元。将阿替利珠单抗-贝伐珠单抗的价格降低20%和29%将满足150,000美元/QALY和100,000美元/QALY的支付意愿阈值。此外,将治疗持续时间限制在≤12个月或降低贝伐珠单抗的剂量至≤10 mg/kg将使阿替利珠单抗-贝伐珠单抗具有成本效益。
阿替利珠单抗-贝伐珠单抗的长期有效性是其成本效益的关键但不确定的决定因素。即使长期临床结局一般,降价也将对成本效益产生有利影响。有必要进一步研究以优化治疗的持续时间和剂量。