Paidi Suresh Kumar, Nair Krishna Kumar Mohanan, Namboodiri Narayanan, Balaguru Sridhar, Valaparambil Ajitkumar
Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India.
Ann Pediatr Cardiol. 2021 Jan-Mar;14(1):107-112. doi: 10.4103/apc.APC_84_20. Epub 2020 Nov 25.
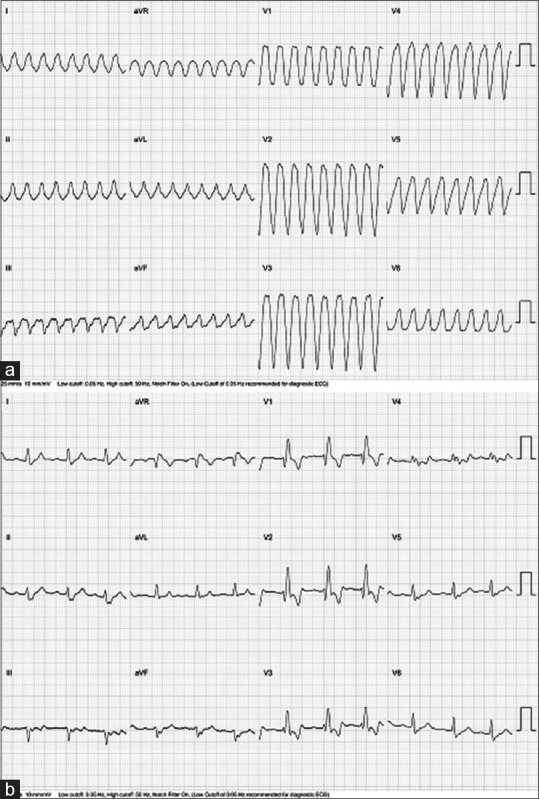
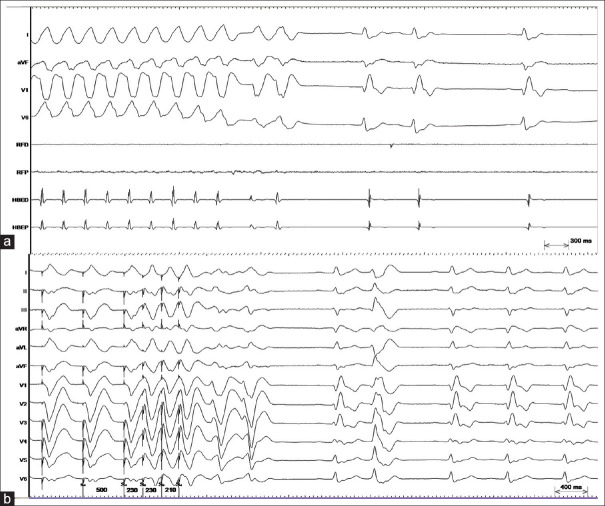
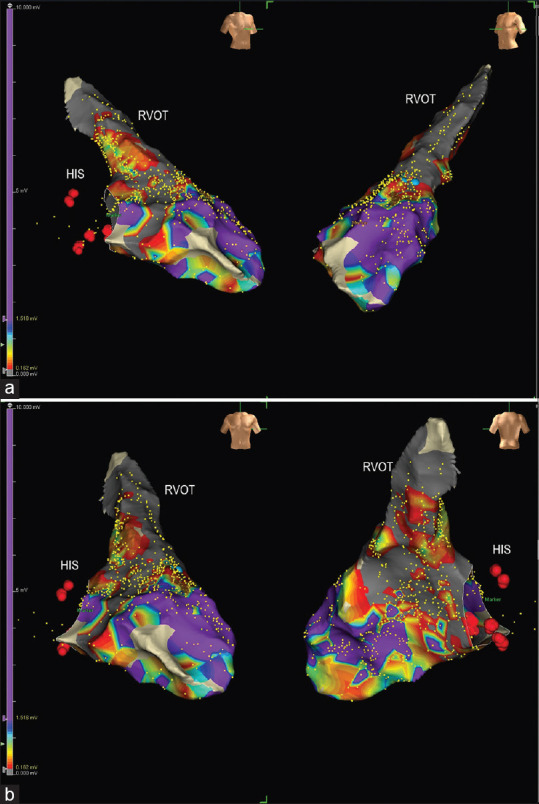
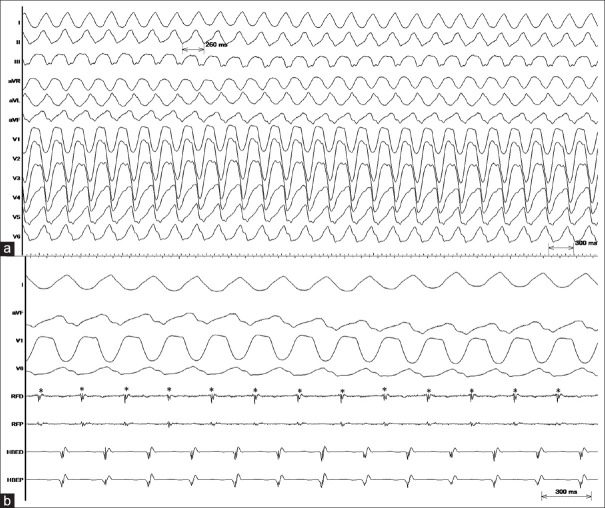
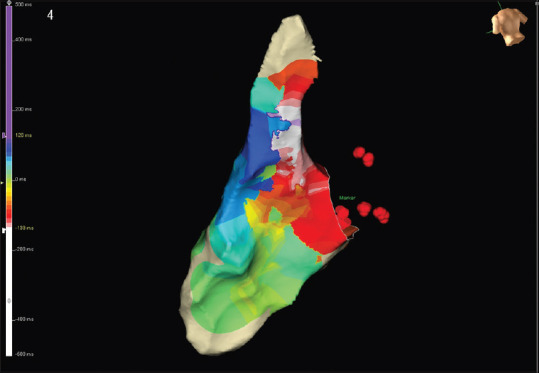
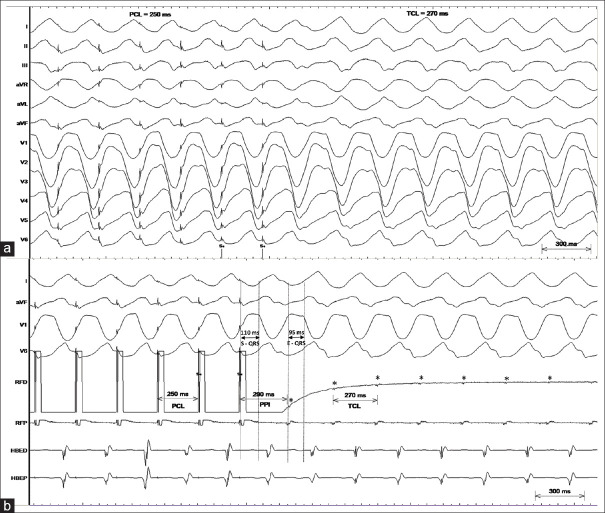
A 47-year-old female underwent cardiac repair for tetralogy of Fallot at the age of 12 years. Subsequently, she was asymptomatic on follow-up. Recently, she presented elsewhere with palpitations and presyncope with documented ventricular tachycardia (VT) having left bundle branch block morphology with inferior QRS axis and late precordial transition. She was reported to have cardioverted and referred to our center for electrophysiology study (EP). She underwent EP study which induced clinical VT which was hemodynamically stable and the mechanism of VT was confirmed as re-entry. With the help of three-dimensional mapping system, VT circuit was identified in the posterior right ventricular outflow tract region between the pulmonary valve and upper end of ventricular septal defect patch. Delivery of radiofrequency energy during VT terminated the tachycardia with no further inducible VT despite aggressive pacing protocols.
一名47岁女性12岁时因法洛四联症接受了心脏修复手术。术后随访期间她无症状。最近,她因心悸和前驱晕厥前往其他地方就诊,记录显示有室性心动过速(VT),呈左束支传导阻滞形态,QRS电轴下偏且胸前导联过渡延迟。据报告她已复律,并转诊至我们中心进行电生理研究(EP)。她接受了EP研究,诱发了血流动力学稳定的临床VT,VT机制被确认为折返。借助三维标测系统,在肺动脉瓣和室间隔缺损补片上端之间的右心室流出道后部区域确定了VT环路。在VT发作期间进行射频能量传递终止了心动过速,尽管采用了积极的起搏方案,仍未再诱发VT。