Zhu Siji, Li Yafen, Chen Weiguo, Fei Xiaochun, Shen Kunwei, Chen Xiaosong
Department of General Surgery, Comprehensive Breast Health Center, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Department of Pathology, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Front Oncol. 2021 Feb 19;11:636266. doi: 10.3389/fonc.2021.636266. eCollection 2021.
Breast cancer (BC) patients with T1N0 tumors have relatively favorable clinical outcomes. However, it remains unclear whether molecular subtypes can aide in prognostic prediction for such small, nodal-negative BC cases and guide decision-making about escalating or de-escalating treatments.
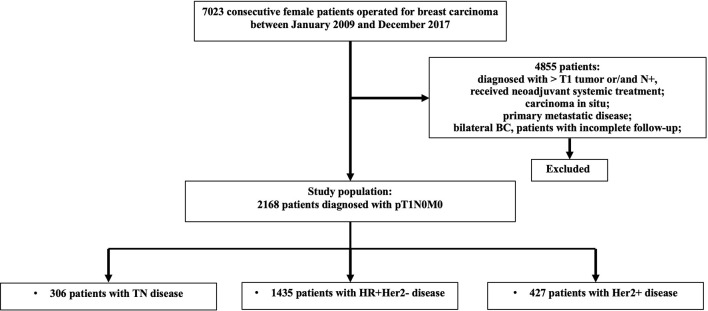
T1N0 BC patients diagnosed between 2009 and 2017 were included and classified into three subgroups according to receptor status: 1) hormonal receptor (HR)+/human epidermal growth factor receptor-2 (HER2)-; 2) HER2+; and 3) triple negative (TN) (HR-/HER2-). Patients' characteristics and relapse events were reviewed. Kaplan-Meier analysis and Cox regression were used to assess the iDFS and BCSS. The effects of risk factors and adjuvant treatment benefits were evaluated by calculating hazard ratios (HRs) for invasive disease-free survival (iDFS) and breast cancer-specific survival (BCSS) with Cox proportional hazards models.
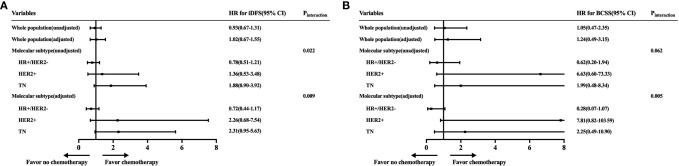
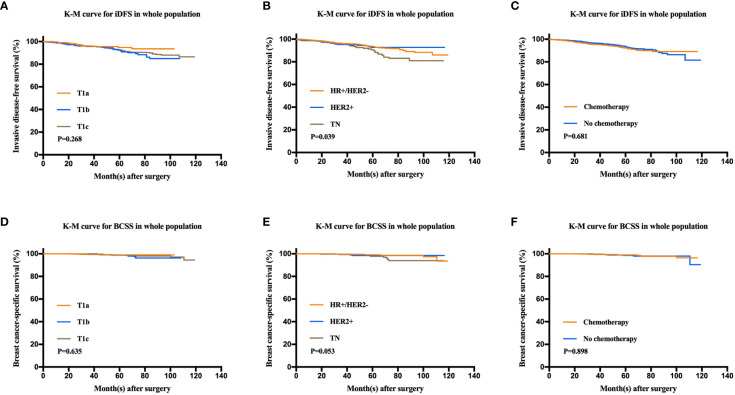
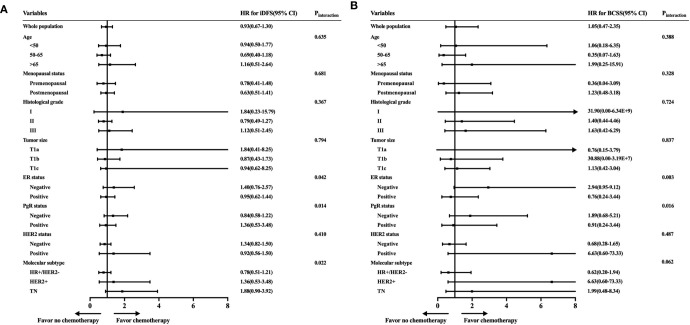
In total, 2,168 patients (1,435 HR+/HER2-, 427 HER2+, 306 TN) were enrolled. The 5-year iDFS rates were 93.6, 92.7, and 90.6% for HR+/HER2-, HER2+, and TN patients, respectively (P = 0.039). Multivariate analysis demonstrated that molecular subtype (P = 0.043), but not tumor size (P = 0.805), was independently associated with iDFS in T1N0 BC. TN patients [HRs = 1.77, 95% confidence interval (CI) = 1.11-2.84, P = 0.018] had a higher recurrence risk than HR+/HER2- patients. Adjuvant chemotherapy benefit was not demonstrated in all T1N0 patients but interacted with molecular subtype status. TN (adjusted HRs = 2.31, 95% CI = 0.68-7.54) and HER2+ (adjusted HRs = 2.26, 95% CI = 0.95-5.63) patients receiving chemotherapy had superior iDFS rates. Regarding BCSS, molecular subtype tended to be related to outcome (P = 0.053) and associated with chemotherapy benefit (P = 0.005).
Molecular subtype was more associated with disease outcome and chemotherapy benefit than tumor size in T1N0 BC patients, indicating that it may guide possible clinical de-escalating therapy in T1N0 BC.
T1N0期肿瘤的乳腺癌(BC)患者具有相对良好的临床预后。然而,分子亚型是否有助于对此类微小、无淋巴结转移的BC病例进行预后预测,并指导关于强化或弱化治疗的决策,仍不清楚。
纳入2009年至2017年间诊断的T1N0期BC患者,并根据受体状态分为三个亚组:1)激素受体(HR)+/人表皮生长因子受体2(HER2)-;2)HER2+;3)三阴性(TN)(HR-/HER2-)。回顾患者的特征和复发事件。采用Kaplan-Meier分析和Cox回归评估无侵袭性疾病生存期(iDFS)和乳腺癌特异性生存期(BCSS)。通过计算侵袭性疾病无进展生存期(iDFS)和乳腺癌特异性生存期(BCSS)的风险比(HRs),利用Cox比例风险模型评估危险因素和辅助治疗的益处。
共纳入2168例患者(1435例HR+/HER2-,427例HER2+,306例TN)。HR+/HER2-、HER2+和TN患者的5年iDFS率分别为93.6%、92.7%和90.6%(P = 0.039)。多因素分析表明,分子亚型(P = 0.043)而非肿瘤大小(P = 0.805)与T1N0期BC的iDFS独立相关。TN患者[HRs = 1.77,95%置信区间(CI)= 1.11 - 2.84,P = 0.018]的复发风险高于HR+/HER2-患者。并非所有T1N0期患者都显示辅助化疗有益,但辅助化疗益处与分子亚型状态存在交互作用。接受化疗的TN患者(调整后HRs = 2.31,95% CI = 0.68 - 7.54)和HER2+患者(调整后HRs = 2.26,95% CI = 0.95 - 5.63)的iDFS率更高。关于BCSS,分子亚型倾向于与预后相关(P = 0.053)且与化疗益处相关(P = 0.005)。
在T1N0期BC患者中,分子亚型比肿瘤大小更能影响疾病预后和化疗益处,这表明它可能指导T1N0期BC患者进行可能的临床弱化治疗。