Department of Cardiovascular Surgery Mount Sinai Hospital New York NY.
Division of Cardiac Surgery Brigham and Women's Hospital Boston MA.
J Am Heart Assoc. 2021 Mar 16;10(6):e019854. doi: 10.1161/JAHA.120.019854. Epub 2021 Mar 9.
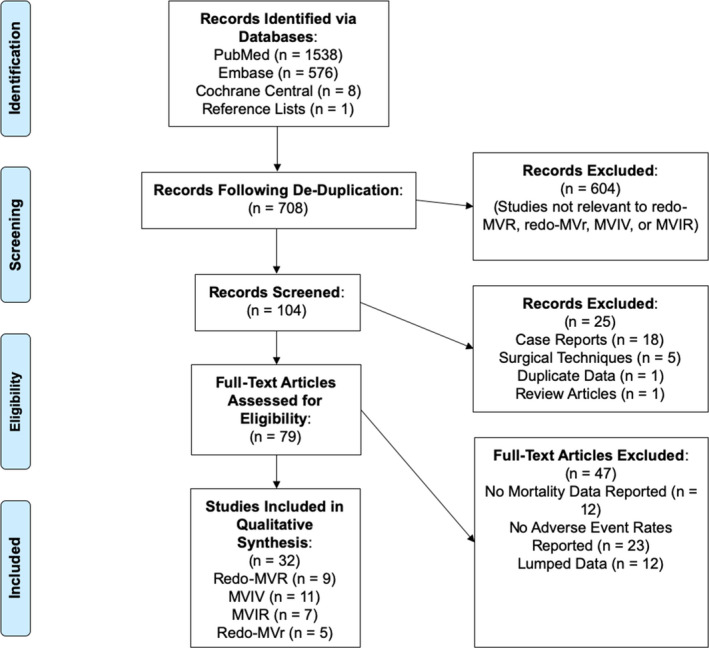
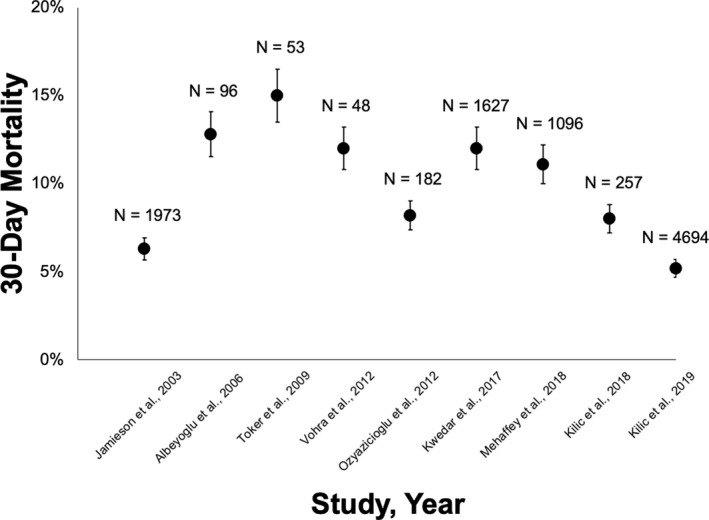
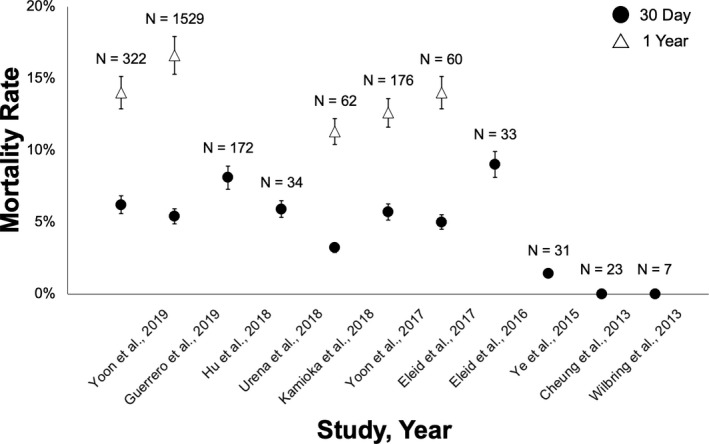
Bioprosthetic mitral structural valve degeneration and failed mitral valve repair (MVr) have traditionally been treated with reoperative mitral valve surgery. Transcatheter mitral valve-in-valve (MVIV) and valve-in-ring (MVIR) replacement are now feasible, but data comparing these approaches are lacking. We sought to compare the outcomes of (1) reoperative mitral valve replacement (redo-MVR) and MVIV for structural valve degeneration, and (2) reoperative mitral valve repair (redo-MVr) or MVR and MVIR for failed MVr. A literature search of PubMed, Embase, and the Cochrane Library was conducted up to July 31, 2020. Thirty-two studies involving 25 832 patients were included. Redo-MVR was required in ≈35% of patients after index surgery at 10 years, with 5% to 15% 30-day mortality. MVIV resulted in >95% procedural success with 30-day and 1-year mortality of 0% to 8% and 11% to 16%, respectively. Recognized complications included left ventricular outflow tract obstruction (0%-6%), valve migration (0%-9%), and residual regurgitation (0%-6%). Comparisons of redo-MVR and MVIV showed no statistically significant differences in mortality (11.3% versus 11.9% at 1 year, =0.92), albeit higher rates of major bleeding and arrhythmias with redo-MVR. MVIR resulted in 0% to 34% mortality at 1 year, whereas both redo-MVr and MVR for failed repairs were performed with minimal mortality and durable long-term results. MVIV is therefore a viable alternative to redo-MVR for structural valve degeneration, whereas redo-MVr or redo-MVR is preferred for failed MVr given the suboptimal results with MVIR. However, not all patients will be candidates for MVIV/MVIR because anatomical restrictions may preclude transcatheter options from adequately addressing the underlying pathology.
生物瓣二尖瓣结构瓣退化和二尖瓣修复术(MVr)失败传统上采用再次二尖瓣手术治疗。经导管二尖瓣瓣中瓣(MVIV)和瓣中环(MVIR)置换现在已经可行,但缺乏这些方法比较的数据。我们旨在比较(1)结构性瓣退化的再次二尖瓣置换(redo-MVR)和 MVIV 以及(2)二尖瓣修复术失败的再次二尖瓣修复(redo-MVr)或 MVR 和 MVIR 的结果。对 PubMed、Embase 和 Cochrane Library 进行了文献检索,截至 2020 年 7 月 31 日。共纳入 32 项涉及 25832 例患者的研究。首次手术后 10 年,约 35%的患者需要再次行 MVR,30 天死亡率为 5%至 15%。MVIV 的手术成功率>95%,30 天和 1 年死亡率分别为 0%至 8%和 11%至 16%。公认的并发症包括左心室流出道梗阻(0%至 6%)、瓣环迁移(0%至 9%)和残余反流(0%至 6%)。与 redo-MVR 相比,MVIV 组的死亡率无统计学显著差异(1 年时为 11.3%与 11.9%,=0.92),尽管 redo-MVR 组的主要出血和心律失常发生率较高。MVIR 在 1 年时的死亡率为 0%至 34%,而 redo-MVr 和 MVR 治疗失败修复的死亡率均较低,且长期结果持久。因此,对于结构性瓣退化,MVIV 是 redo-MVR 的可行替代方法,而对于二尖瓣修复术失败,由于 MVIR 的结果不理想,因此首选 redo-MVr 或 redo-MVR。然而,并非所有患者都适合接受 MVIV/MVIR 治疗,因为解剖学限制可能会使经导管方法无法充分解决潜在的病理问题。