Leukemia Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY.
Weill Cornell Medical College, New York, NY; and.
Blood Adv. 2021 Mar 9;5(5):1552-1564. doi: 10.1182/bloodadvances.2020003734.
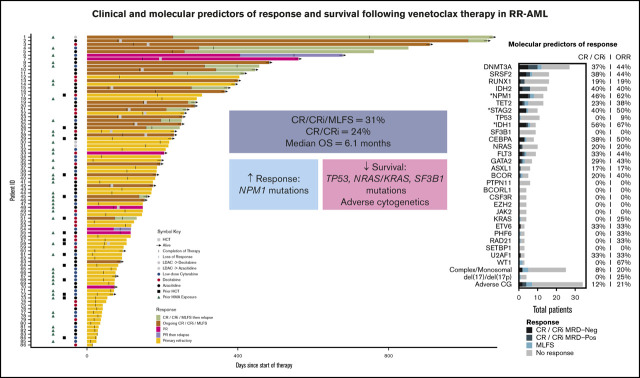
Azacitidine + venetoclax, decitabine + venetoclax, and low-dose cytarabine + venetoclax are now standard treatments for newly diagnosed older or unfit patients with acute myeloid leukemia (AML). Although these combinations are also commonly used in relapsed or refractory AML (RR-AML), clinical and molecular predictors of response and survival in RR-AML are incompletely understood. We retrospectively analyzed clinical and molecular characteristics and outcomes for 86 patients with RR-AML who were treated with venetoclax combinations. The complete remission (CR) or CR with incomplete hematologic recovery (CRi) rate was 24%, and the overall response rate was 31% with the inclusion of a morphologic leukemia-free state. Azacitidine + venetoclax resulted in higher response rates compared with low-dose cytarabine + venetoclax (49% vs 15%; P = .008). Median overall survival (OS) was 6.1 months, but it was significantly longer with azacitidine + venetoclax compared with low-dose cytarabine + venetoclax (25 vs 3.9 months; P = .003). This survival advantage of azacitidine + venetoclax over low-dose cytarabine + venetoclax persisted when patients were censored for subsequent allogeneic stem cell transplantation (8.1 vs 3.9 months; P = .035). Mutations in NPM1 were associated with higher response rates, whereas adverse cytogenetics and mutations in TP53, KRAS/NRAS, and SF3B1 were associated with worse OS. Relapse was driven by diverse mechanisms, including acquisition of novel mutations and an increase in cytogenetic complexity. Venetoclax combination therapy is effective in many patients with RR-AML, and pretreatment molecular characteristics may predict outcomes. Trials that evaluate novel agents in combination with venetoclax therapy in patients with RR-AML that have adverse risk genomic features are warranted.
阿扎胞苷+维奈托克、地西他滨+维奈托克和低剂量阿糖胞苷+维奈托克现在是新诊断的老年或不适合治疗的急性髓系白血病(AML)患者的标准治疗方法。虽然这些联合方案也常用于复发或难治性 AML(RR-AML),但 RR-AML 患者对这些联合方案的反应和生存的临床和分子预测因素仍不完全清楚。我们回顾性分析了 86 例接受维奈托克联合方案治疗的 RR-AML 患者的临床和分子特征及结果。完全缓解(CR)或不完全血液学恢复的 CR(CRi)率为 24%,包括形态学白血病无状态在内的总反应率为 31%。阿扎胞苷+维奈托克的反应率高于低剂量阿糖胞苷+维奈托克(49% vs. 15%;P =.008)。中位总生存期(OS)为 6.1 个月,但阿扎胞苷+维奈托克组明显长于低剂量阿糖胞苷+维奈托克组(25 个月 vs. 3.9 个月;P =.003)。当对接受后续异基因造血干细胞移植的患者进行删失时,阿扎胞苷+维奈托克相对于低剂量阿糖胞苷+维奈托克的生存优势仍然存在(8.1 个月 vs. 3.9 个月;P =.035)。NPM1 突变与更高的反应率相关,而不良细胞遗传学和 TP53、KRAS/NRAS 和 SF3B1 突变与更差的 OS 相关。复发是由多种机制驱动的,包括获得新的突变和细胞遗传学复杂性增加。维奈托克联合治疗在许多 RR-AML 患者中有效,治疗前的分子特征可能预测结局。在 RR-AML 患者中,有不良风险基因组特征的患者,评估新型药物与维奈托克联合治疗的临床试验是必要的。