Kobayashi Tomoaki, Sotomi Yohei, Hirata Akio, Sakata Yasushi, Hirayama Atsushi, Higuchi Yoshiharu
Department of Cardiology, Osaka Police Hospital Osaka Japan.
Department of Cardiovascular Medicine, Osaka University Graduate School of Medicine Osaka Japan.
Circ Rep. 2020 Apr 7;2(6):289-296. doi: 10.1253/circrep.CR-20-0026.
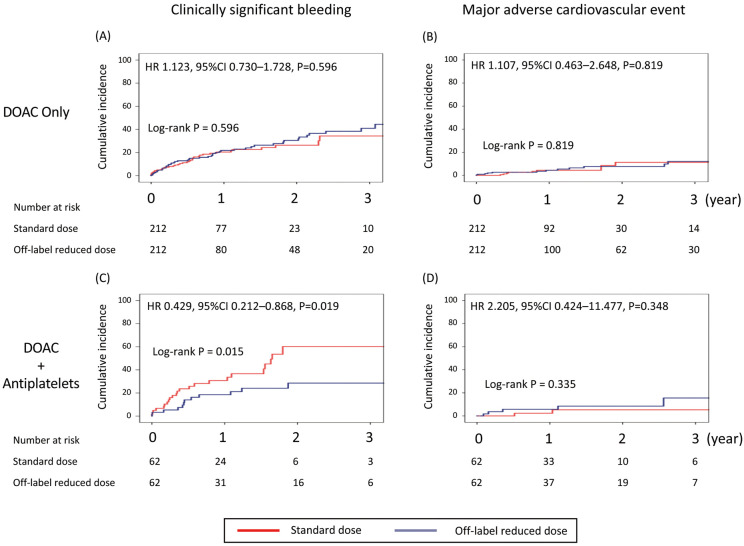
The association between direct oral anticoagulant (DOAC) dose and clinical outcomes when used with antiplatelets still remains to be investigated. We conducted a prospective registry of non-valvular atrial fibrillation (AF) patients with DOAC: the DIRECT registry (n=2,216; follow-up, 407±388 days). We analyzed patients taking standard dose (n=907) and off-label reduced dose (n=338) DOAC in this sub-analysis. These patients were further stratified by add-on antiplatelets. Because DOAC dose was not randomly selected, potential confounding factors were eliminated through a propensity score-matching technique. The primary endpoint was clinically significant bleeding. The secondary endpoint was major adverse cardiovascular events (MACE; composite of all-cause death, all myocardial infarction, and stroke/systemic embolism). In patients with DOAC only/DOAC+antiplatelets, we successfully matched 212/62 patients who received off-label reduced dose DOAC with 212/62 standard dose patients. Off-label DOAC dose reduction did not have a significant impact on bleeding (HR, 1.123; 95% CI: 0.730-1.728, P=0.596) or MACE (HR, 1.107; 95% CI: 0.463-2.648, P=0.819) in patients with DOAC only, whereas in patients with add-on antiplatelets, off-label dose reduction significantly reduced bleeding (HR, 0.429; 95% CI: 0.212-0.868, P=0.019) without increasing MACE (HR, 2.205; 95% CI: 0.424-11.477, P=0.348). Reduced DOAC dose in combination with antiplatelet agents was associated with fewer bleeding complications than standard-dose therapy with no reduction in efficacy.
直接口服抗凝剂(DOAC)与抗血小板药物联合使用时,其剂量与临床结局之间的关联仍有待研究。我们对使用DOAC的非瓣膜性心房颤动(AF)患者进行了一项前瞻性登记研究:DIRECT登记研究(n = 2216;随访时间为407±388天)。在本次亚分析中,我们分析了服用标准剂量(n = 907)和非标准降低剂量(n = 338)DOAC的患者。这些患者根据是否加用抗血小板药物进一步分层。由于DOAC剂量并非随机选择,因此通过倾向评分匹配技术消除了潜在的混杂因素。主要终点是具有临床意义的出血。次要终点是主要不良心血管事件(MACE;全因死亡、所有心肌梗死以及中风/全身性栓塞的复合事件)。在仅使用DOAC/DOAC +抗血小板药物的患者中,我们成功将212/62例接受非标准降低剂量DOAC的患者与212/62例标准剂量患者进行了匹配。在仅使用DOAC的患者中,非标准DOAC剂量降低对出血(HR,1.123;95%CI:0.730 - 1.728,P = 0.596)或MACE(HR,1.107;95%CI:0.463 - 2.648,P = 0.819)没有显著影响,而在加用抗血小板药物的患者中,非标准剂量降低显著减少了出血(HR,0.429;95%CI:0.212 - 0.868,P = 0.019),且未增加MACE(HR,2.205;95%CI:0.424 - 11.477,P = 0.348)。与标准剂量治疗相比,DOAC降低剂量联合抗血小板药物与更少的出血并发症相关,且疗效未降低。