University of Illinois at Chicago, IL, USA.
Neurorehabil Neural Repair. 2021 Apr;35(4):367-378. doi: 10.1177/1545968321999049. Epub 2021 Mar 11.
Stroke rehabilitation may be improved with a better understanding of the contribution of ipsilateral motor pathways to the paretic limb and alterations in transcallosal inhibition. Few studies have evaluated these factors during dynamic, bilateral lower limb movements, and it is unclear whether they relate to functional outcomes.
Determine if lower limb ipsilateral excitability and transcallosal inhibition after stroke depend on target limb, task, or number of limbs involved, and whether these factors are related to clinical measures.
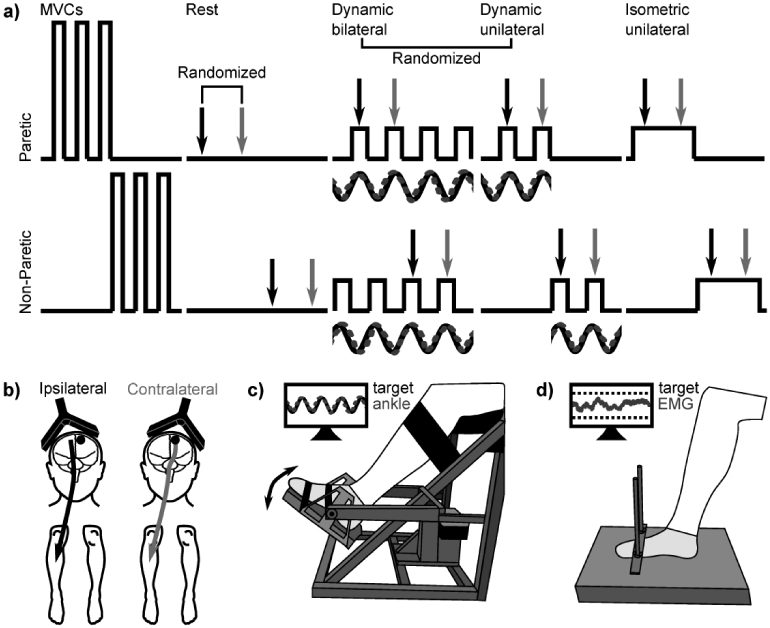
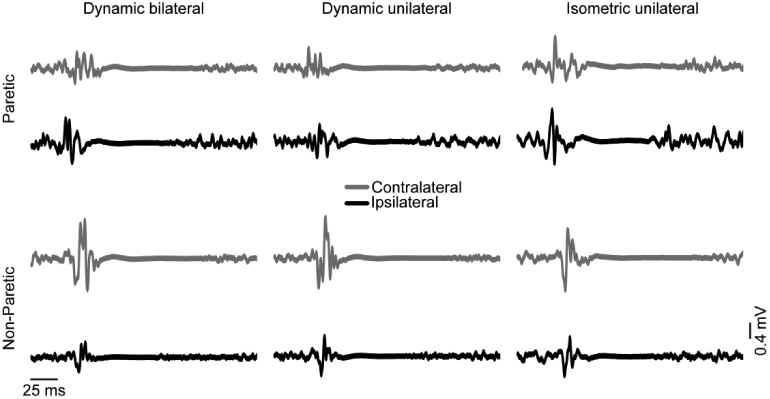
In 29 individuals with stroke, ipsilateral and contralateral responses to transcranial magnetic stimulation were measured in the paretic and nonparetic tibialis anterior during dynamic (unilateral or bilateral ankle dorsiflexion/plantarflexion) and isometric (unilateral dorsiflexion) conditions. Relative ipsilateral excitability and transcallosal inhibition were assessed. Fugl-Meyer, ankle movement accuracy, and walking characteristics were assessed.
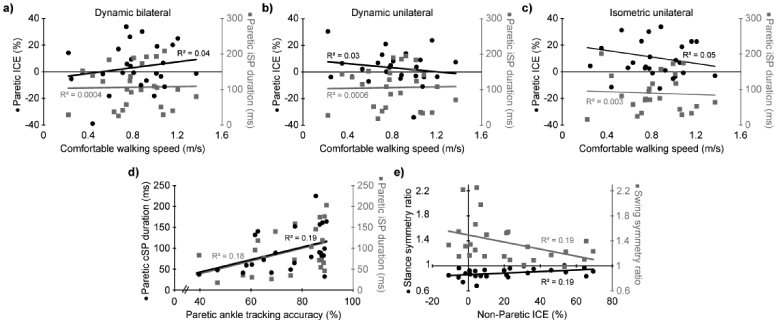
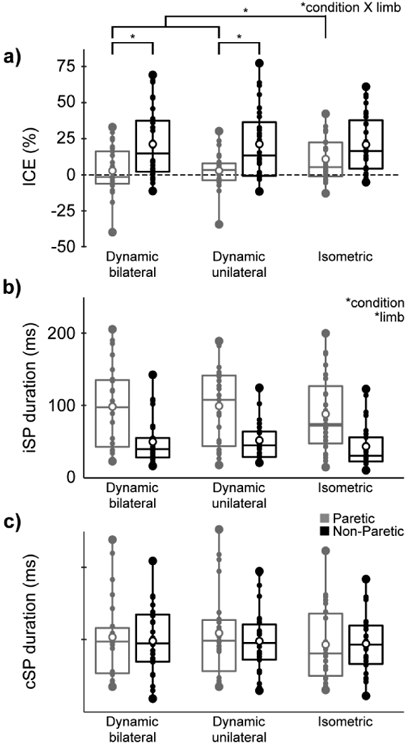
Relative ipsilateral excitability was greater during dynamic than isometric conditions in the paretic limb ( ≤ .02) and greater in the paretic than the nonparetic limb during dynamic conditions ( ≤ .004). Transcallosal inhibition was greater in the ipsilesional than contralesional hemisphere ( = .002) and during dynamic than isometric conditions ( = .03). Greater ipsilesional transcallosal inhibition was correlated with better ankle movement accuracy ( = 0.18, = .04). Greater contralateral excitability to the nonparetic limb was correlated with improved walking symmetry ( = 0.19, = .03).
Ipsilateral pathways have increased excitability to the paretic limb, particularly during dynamic tasks. Transcallosal inhibition is greater in the ipsilesional than contralesional hemisphere and during dynamic than isometric tasks. Ipsilateral pathways and transcallosal inhibition may influence walking asymmetry and ankle movement accuracy.
通过更好地了解患侧运动通路对瘫痪肢体的贡献以及皮质内抑制的改变,可能会改善中风康复。很少有研究评估这些因素在动态双侧下肢运动期间的情况,也不清楚它们是否与功能结果有关。
确定中风后下肢同侧兴奋性和皮质内抑制是否取决于目标肢体、任务或涉及的肢体数量,以及这些因素是否与临床测量值有关。
在 29 名中风患者中,在动态(单侧或双侧踝关节背屈/跖屈)和等长(单侧背屈)条件下,测量瘫痪和非瘫痪胫骨前肌的经颅磁刺激对侧和同侧反应。评估相对同侧兴奋性和皮质内抑制。评估 Fugl-Meyer、踝关节运动准确性和步行特征。
在瘫痪肢体中,动态条件下的同侧兴奋性(与等长条件相比)大于等长条件(≤0.02),且在动态条件下的瘫痪肢体中大于非瘫痪肢体(≤0.004)。同侧皮质内抑制在优势半球大于对侧半球(=0.002),在动态条件下大于等长条件(=0.03)。更大的同侧皮质内抑制与更好的踝关节运动准确性相关(=0.18,=0.04)。非瘫痪肢体的对侧兴奋性增加与步行对称性改善相关(=0.19,=0.03)。
患侧通路对瘫痪肢体的兴奋性增加,尤其是在动态任务中。同侧皮质内抑制在优势半球大于对侧半球,在动态条件下大于等长条件。同侧通路和皮质内抑制可能会影响步行不对称性和踝关节运动准确性。