Stromberger Carmen, Yedikat Berna, Coordes Annekatrin, Tinhofer Ingeborg, Kalinauskaite Goda, Budach Volker, Zschaeck Sebastian, Raguse Jan-Dirk, Kofla Grzegorz, Heiland Max, Stsefanenka Aksana, Beck-Broichsitter Benedicta, Dommerich Steffen, Senger Carolin, Beck Marcus
Department of Radiation Oncology, Charité-Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin, Germany.
Berlin Institute of Health (BIH), Berlin, Germany.
Front Oncol. 2021 Feb 23;10:566318. doi: 10.3389/fonc.2020.566318. eCollection 2020.
Older patients with head and neck cancer (HNC) represent a challenging group, as frailty and comorbidities need to be considered. This study aimed to evaluate the efficacy and side effects of curative and palliative (chemo) radiation ([C]RT) with regard to basic geriatric screening in older patients.
This study included HNC patients aged ≥70 years who were treated with curative or palliative (C)RT. Clinicopathological data including Charlson Comorbidity Index (CCI), Karnofsky performance status (KPS), and treatment data were analyzed as predictors of overall survival (OS).
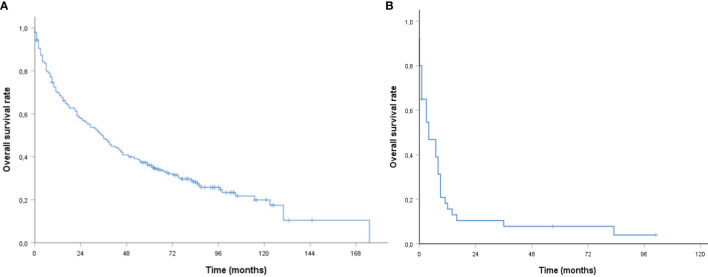
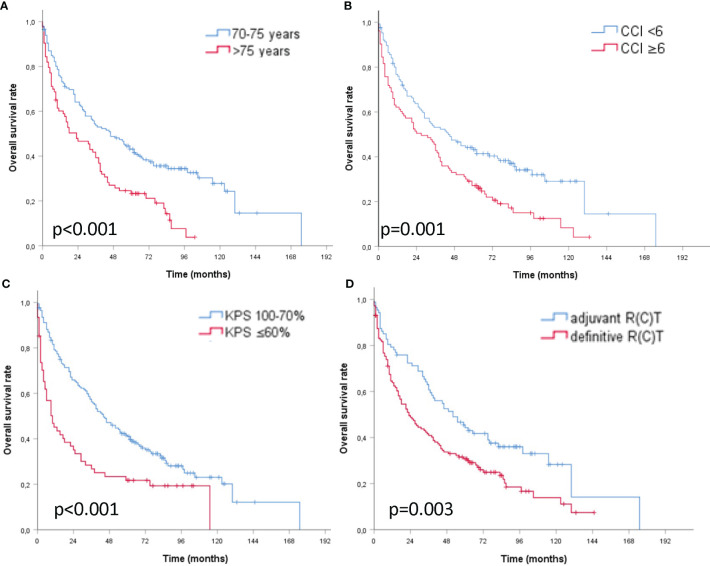
A total of 271 patients (median age, 74 years) were enrolled. The majority had UICC stage III/IV (90%) and underwent curative treatment (85.2%). A total of 144 (53.1%) patients received definitive and 87 (32.1%) had adjuvant (C)RT. Overall, 40 patients (14.8%) received palliative (C)RT. Median follow-up duration (curative setting) was 87 months, and the 2- and 5-year OS rates were 57.8 and 35.9%, respectively. Median OS was significantly different for age ≤75 >75 years, CCI <6 ≥6, KPS ≥70 <70%, Tx/T1/T2 v. T3/T4, and adjuvant definitive (C)RT, respectively. Age 70-75 years (p = 0.004), fewer comorbidities when CCI < 6 (p = 0.014), good KPS ≥ 70% (p = 0.001), and adjuvant (C)RT (p = 0.008) independently predicted longer survival. Palliative RT resulted in a median OS of 4 months.
Older age, lower KPS, higher CCI, and definitive (C)RT are indicators of worse survival in older patients with HNC treated curatively. Without a comprehensive geriatric assessment in patients aged >75 years, the KPS and CCI can be useful tools to account for "fitness, vulnerability or frailty" to help in treatment decision-making.
老年头颈癌(HNC)患者是一个具有挑战性的群体,因为需要考虑其身体虚弱和合并症情况。本研究旨在评估根治性和姑息性(化疗)放疗([C]RT)对老年患者进行基本老年筛查的疗效和副作用。
本研究纳入了年龄≥70岁且接受根治性或姑息性(C)RT治疗的HNC患者。分析包括Charlson合并症指数(CCI)、卡诺夫斯基功能状态(KPS)在内的临床病理数据以及治疗数据,作为总生存期(OS)的预测指标。
共纳入271例患者(中位年龄74岁)。大多数患者为国际抗癌联盟(UICC)III/IV期(90%),并接受了根治性治疗(85.2%)。共有144例(53.1%)患者接受了根治性放疗,87例(32.1%)接受了辅助性(C)RT。总体而言,40例(14.8%)患者接受了姑息性(C)RT。中位随访时间(根治性治疗组)为87个月,2年和5年总生存率分别为57.8%和35.9%。年龄≤75岁与>75岁、CCI<6与≥6、KPS≥70%与<70%、Tx/T1/T2与T3/T4以及辅助性与根治性(C)RT的中位总生存期均有显著差异。年龄70 - 75岁(p = 0.004)、CCI<6时合并症较少(p = 0.014)、良好的KPS≥70%(p = 0.001)以及辅助性(C)RT(p = 0.008)独立预测生存期更长。姑息性放疗的中位总生存期为4个月。
年龄较大、KPS较低、CCI较高以及根治性(C)RT是接受根治性治疗的老年HNC患者生存较差的指标。对于年龄>75岁的患者,若未进行全面的老年评估,则KPS和CCI可作为评估“健康状况、脆弱性或身体虚弱程度”的有用工具,以帮助进行治疗决策。