Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Department of Surgical, Medical, Molecular and Critical Area Pathology, University of Pisa, Pisa, Italy.
BMC Med. 2021 Mar 15;19(1):66. doi: 10.1186/s12916-021-01936-3.
It is unclear whether insulin resistance (IR) contributes to excess mortality in patients with type 2 diabetes independent of diabetic kidney disease (DKD), which is strongly associated with IR and is a major risk factor for cardiovascular disease (CVD), the main cause of death in these individuals. We tested this hypothesis in patients with type 2 diabetes from the Renal Insufficiency And Cardiovascular Events Italian Multicentre Study.
This observational, prospective, cohort study enrolled 15,773 patients with type 2 diabetes attending 19 Italian Diabetes Clinics in 2006-2008. Insulin sensitivity was assessed as estimated glucose disposal rate (eGDR), which was validated against the euglycaemic-hyperinsulinemic clamp technique. Vital status on October 31, 2015, was retrieved for 15,656 patients (99.3%). Participants were stratified by eGDR tertiles from T1 (≥ 5.35 mg/kg/min) to T3 (≤ 4.14 mg/kg/min, highest IR).
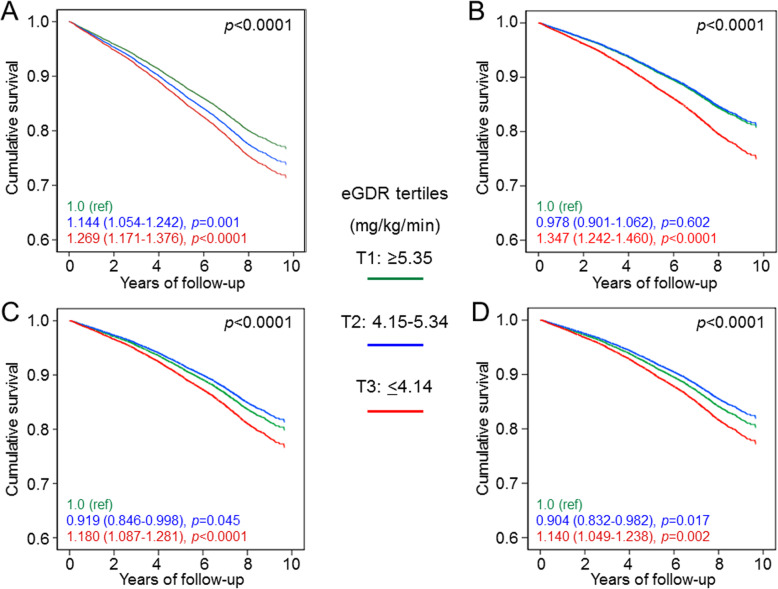
CVD risk profile was worse in T2 and T3 vs T1. eGDR tertiles were independently associated with micro- and macroalbuminuria and the albuminuric DKD phenotypes (albuminuria with preserved or reduced estimated glomerular filtration rate [eGFR]) as well as with eGFR categories or the nonalbuminuric DKD phenotype. Over a 7.4-year follow-up, unadjusted death rates and mortality risks increased progressively across eGDR tertiles, but remained significantly elevated after adjustment only in T3 vs T1 (age- and gender- adjusted death rate, 22.35 vs 16.74 per 1000 person-years, p < 0.0001, and hazard ratio [HR] adjusted for multiple confounders including DKD, 1.140 [95% confidence interval [CI], 1.049-1.238], p = 0.002). However, eGDR was independently associated with mortality in participants with no DKD (adjusted HR, 1.214 [95% CI, 1.072-1.375], p = 0.002) and in those with nonalbuminuric DKD (1.276 [1.034-1.575], p = 0.023), but not in those with the albuminuric DKD phenotypes. Moreover, the association was stronger in males and in younger individuals and was observed in those without but not with prior CVD, though interaction was significant only for age.
The proxy of insulin sensitivity eGDR predicts all-cause mortality in type 2 diabetes, independent of confounders including DKD. However, the impact of IR in individuals with albuminuric DKD may be mediated by its relationship with albuminuria.
ClinicalTrials.gov , NCT00715481, retrospectively registered 15 July 2008.
目前尚不清楚 2 型糖尿病患者的胰岛素抵抗(IR)是否独立于糖尿病肾病(DKD)导致死亡率增加,而 DKD 与 IR 密切相关,是心血管疾病(CVD)的主要危险因素,也是这些患者的主要死亡原因。我们在来自意大利肾脏和心血管事件多中心研究的 2 型糖尿病患者中检验了这一假说。
这是一项观察性、前瞻性队列研究,纳入了 2006 年至 2008 年期间在意大利 19 家糖尿病诊所就诊的 15773 例 2 型糖尿病患者。胰岛素敏感性通过估计葡萄糖处置率(eGDR)来评估,该指标已通过葡萄糖钳夹技术得到验证。截至 2015 年 10 月 31 日,15656 例患者(99.3%)的生存状态可获得。根据 eGDR 三分位值(从 T1[≥5.35mg/kg/min]到 T3[≤4.14mg/kg/min,IR 最高])将参与者分层。
与 T1 相比,T2 和 T3 组的 CVD 风险特征更差。eGDR 三分位值与微量白蛋白尿和大量白蛋白尿以及白蛋白尿型 DKD 表型(伴有或不伴有估算肾小球滤过率[eGFR]降低的白蛋白尿)以及 eGFR 类别或非白蛋白尿型 DKD 表型独立相关。在 7.4 年的随访期间,未经校正的死亡率和死亡风险随着 eGDR 三分位值的升高而逐渐升高,但仅在 T3 与 T1 相比仍显著升高(校正年龄和性别后的死亡率,22.35 比 16.74 每 1000 人年,p<0.0001,校正多种混杂因素(包括 DKD)后的危险比[HR],1.140[95%置信区间[CI],1.049-1.238],p=0.002)。然而,在无 DKD 的参与者(校正 HR,1.214[95%CI,1.072-1.375],p=0.002)和非白蛋白尿型 DKD 的参与者(1.276[1.034-1.575],p=0.023)中,eGDR 与死亡率独立相关,但在白蛋白尿型 DKD 表型的参与者中则没有。此外,在男性和较年轻的个体中,这种相关性更强,且仅在没有但不在有既往 CVD 的个体中观察到这种相关性,但交互作用仅在年龄方面有统计学意义。
胰岛素敏感性的替代指标 eGDR 可预测 2 型糖尿病患者的全因死亡率,独立于包括 DKD 在内的混杂因素。然而,在白蛋白尿型 DKD 患者中,IR 的影响可能是通过其与白蛋白尿的关系介导的。
ClinicalTrials.gov,NCT00715481,于 2008 年 7 月 15 日进行了回顾性注册。