Balakrishnan Ashwin S, Hampson Lindsay A, Bell Alexander M, Baghdanian Arthur H, Baghdanian Armonde A, Meng Maxwell V, Odisho Anobel Y
Department of Urology, University of California, San Francisco, CA, USA.
Department of Radiology, University of Southern California, Los Angeles, CA, USA.
Transl Androl Urol. 2021 Feb;10(2):765-774. doi: 10.21037/tau-20-1050.
Reducing surgical supply costs can help to lower hospital expenditures. We aimed to evaluate whether variation in supply costs between urologic surgeons performing both robotic or open partial nephrectomies is associated with differential patient outcomes.
In this retrospective cohort study, we reviewed 399 consecutive robotic (n=220) and open (n=179) partial nephrectomies performed at an academic center. Surgical supply costs were determined at the institution-negotiated rate. Through retrospective review, we identified factors related to case complexity, patient comorbidity, and perioperative outcomes. Two radiologists assigned nephrometry scores to grade tumor complexity. We created univariate and multivariable models for predictors of supply costs, length of stay, and change in serum creatinine.
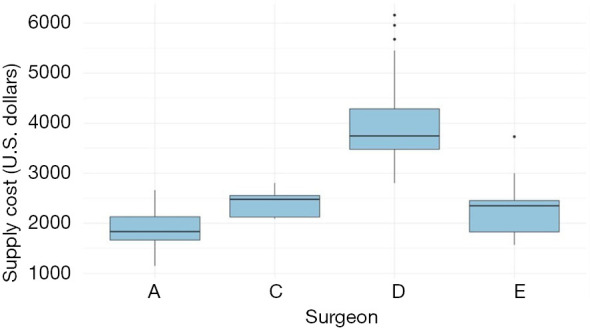
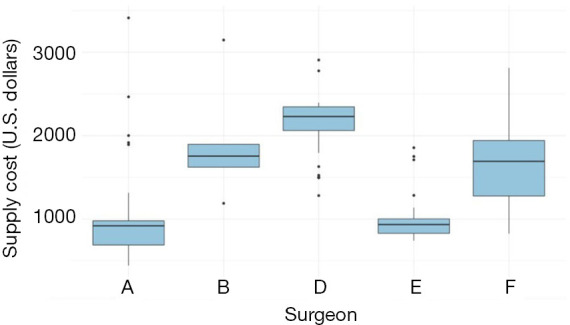
Median supply cost was $3,201 [interquartile range (IQR): $2,201-3,808] for robotic partial nephrectomy and $968 (IQR: $819-1,772) for open partial nephrectomy. Mean nephrometry score was 7.0 (SD =1.7) for robotic procedures and 8.2 (SD =1.6) for open procedures. In multivariable models, the surgeon was the primary significant predictor of variation in surgical supply costs for both procedure types. In multivariable mixed-effects analysis with surgeon as a random effect, supply cost was not a significant predictor of change in serum creatinine for robotic or open procedures. Supply cost was not a statistically significant predictor of length of stay for the open procedure. Supply cost was a significant predictor of longer length of stay for the robotic procedure, however it was not a clinically meaningful change in length of stay (0.02 days per $100 in supply costs).
Higher supply spending did not predict significantly improved patient outcomes. Variability in surgeon supply preference is the likely source of variability in supply cost. These data suggest that efforts to promote cost-effective utilization and standardization of supplies in partial nephrectomy could help reduce costs without harming patients.
降低手术耗材成本有助于降低医院支出。我们旨在评估同时进行机器人辅助或开放性部分肾切除术的泌尿外科医生之间耗材成本的差异是否与不同的患者预后相关。
在这项回顾性队列研究中,我们回顾了在一个学术中心连续进行的399例机器人辅助(n = 220)和开放性(n = 179)部分肾切除术。手术耗材成本按照机构协商的价格确定。通过回顾性分析,我们确定了与病例复杂性、患者合并症和围手术期结局相关的因素。两名放射科医生对肿瘤复杂性进行肾计量评分。我们建立了单变量和多变量模型,用于预测耗材成本、住院时间和血清肌酐变化。
机器人辅助部分肾切除术的中位耗材成本为3201美元[四分位间距(IQR):2201 - 3808美元],开放性部分肾切除术为968美元(IQR:819 - 1772美元)。机器人手术的平均肾计量评分为7.0(标准差 = 1.7),开放手术为8.2(标准差 = 1.6)。在多变量模型中,外科医生是两种手术类型手术耗材成本差异的主要显著预测因素。在以外科医生作为随机效应的多变量混合效应分析中,耗材成本不是机器人辅助或开放手术血清肌酐变化的显著预测因素。耗材成本不是开放手术住院时间的统计学显著预测因素。然而,耗材成本是机器人手术住院时间延长的显著预测因素,但住院时间的变化在临床上并无意义(每100美元耗材成本增加0.02天)。
更高的耗材支出并未预示患者预后显著改善。外科医生对耗材偏好的差异可能是耗材成本差异的来源。这些数据表明,在部分肾切除术中促进耗材的成本效益利用和标准化的努力有助于在不损害患者的情况下降低成本。