Department of Gynecology and Gynecologic Oncology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Department of Gynecology and Gynecologic Oncology, Evang. Kliniken Essen-Mitte, Essen, Germany.
Ann Surg Oncol. 2021 Oct;28(11):6696-6704. doi: 10.1245/s10434-021-09744-y. Epub 2021 Mar 15.
As the population at risk for pelvic nodal involvement remains poorly described, the role of pelvic lymphadenectomy (LAE) in vulvar squamous cell cancer (VSCC) has been a matter of discussion for decades.
In the AGO-CaRE-1 study, 1618 patients with International Federation of Gynecology and Obstetrics (FIGO) stage IB or higher primary VSCC treated at 29 centers in Germany between 1998 and 2008 were documented. In this analysis, only patients with pelvic LAE (n = 70) were analyzed with regard to prognosis and correlation between inguinal and pelvic lymph node involvement.
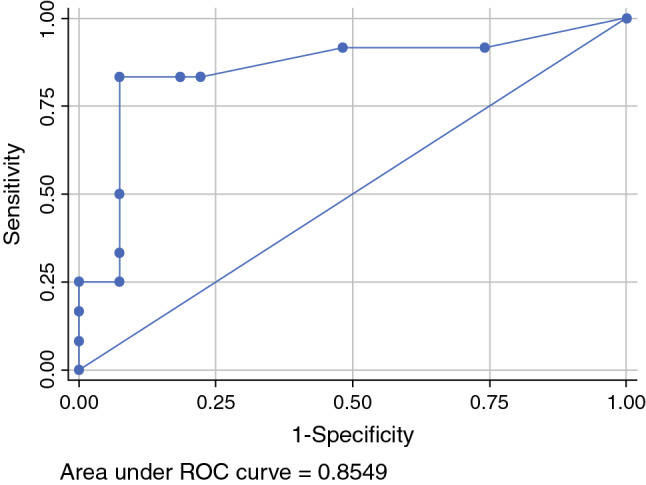
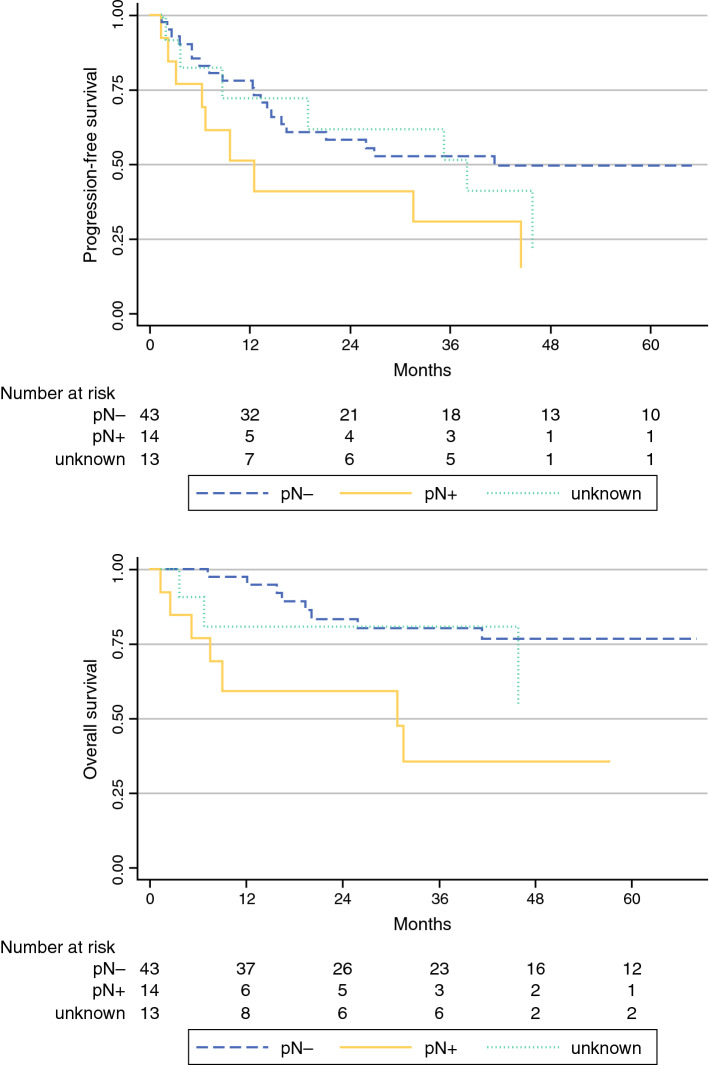
The majority of patients had T1b/T2 tumors (n = 47; 67.1%), with a median diameter of 40 mm (2-240 mm); 54/70 patients (77.1%) who received pelvic LAE had positive groin nodes. For 42 of these 54 patients, the number of affected groin nodes had been documented as a median of 3; 14/42 (33.3%) of these patients had histologically confirmed pelvic nodal metastases (median number of affected pelvic nodes 3 [1-12]). In these 14 patients, the median number of affected groin nodes was 7 (1-30), with a groin metastases median maximum diameter of 42.5 mm (12-50). Receiver operating characteristic analysis showed an area under the curve of 0.85, with 83.3% sensitivity and 92.6% specificity for the prediction of pelvic involvement in cases of six or more positive groin nodes. No cases of pelvic nodal involvement without groin metastases were observed. Prognosis in cases of pelvic metastasis was poor, with a median progression-free survival of only 12.5 months.
For the majority of node-positive patients with VSCC, pelvic nodal staging appears unnecessary since a relevant risk for pelvic nodal involvement only seems to be present in highly node-positive disease.
由于存在盆腔淋巴结转移风险的人群描述不佳,因此盆腔淋巴结清扫术(LAE)在外阴鳞癌(VSCC)中的作用几十年来一直存在争议。
在 AGO-CaRE-1 研究中,记录了 1998 年至 2008 年间德国 29 个中心治疗的国际妇产科联合会(FIGO)分期 IB 期或更高期原发性 VSCC 患者 1618 例。在这项分析中,仅对接受盆腔 LAE(n=70)的患者进行了预后和腹股沟与盆腔淋巴结受累之间的相关性分析。
大多数患者的肿瘤为 T1b/T2 期(n=47;67.1%),肿瘤直径中位数为 40mm(2-240mm);54/70 例(77.1%)接受盆腔 LAE 的患者腹股沟淋巴结阳性。对于这 54 例患者中的 42 例,记录了受影响的腹股沟淋巴结数量中位数为 3;其中 14/42(33.3%)例患者有组织学证实的盆腔淋巴结转移(受影响的盆腔淋巴结数量中位数为 3[1-12])。在这 14 例患者中,受影响的腹股沟淋巴结数量中位数为 7(1-30),腹股沟转移的最大直径中位数为 42.5mm(12-50)。接受者操作特征分析显示曲线下面积为 0.85,当 6 个或更多腹股沟淋巴结阳性时,预测盆腔受累的灵敏度为 83.3%,特异性为 92.6%。未观察到无腹股沟转移的盆腔淋巴结受累的情况。盆腔转移的预后较差,中位无进展生存期仅为 12.5 个月。
对于大多数淋巴结阳性的 VSCC 患者,盆腔淋巴结分期似乎没有必要,因为只有在高度淋巴结阳性疾病中才存在盆腔淋巴结受累的相关风险。