Department of Quantitative Health Sciences, Mayo Clinic, Rochester, Minnesota, USA.
Institute of Sports and Sports Science, Karlsruhe Institute of Technology, Karlsruhe, Germany.
Int J Geriatr Psychiatry. 2021 Sep;36(9):1362-1369. doi: 10.1002/gps.5528. Epub 2021 Mar 24.
Neuropsychiatric symptoms (NPS) are associated with the risk of incident mild cognitive impairment (MCI) and dementia. We examined associations between NPS and the outcomes of global and domain-specific cognitive trajectories.
In this longitudinal study conducted in the setting of the population-based Mayo Clinic Study of Aging, 5081 community-dwelling, nondemented individuals aged ≥50 years (51% males) underwent NPS assessment using Neuropsychiatric Inventory Questionnaire (NPI-Q), and Beck Depression and Anxiety Inventories (BDI-II, BAI). Global and domain-specific (memory, language, attention, and visuospatial skills) cognitive performance was assessed through neuropsychological testing every 15 months. Associations between baseline NPS and trajectories for individual yearly change in cognitive z-scores were calculated using linear mixed-effect models.
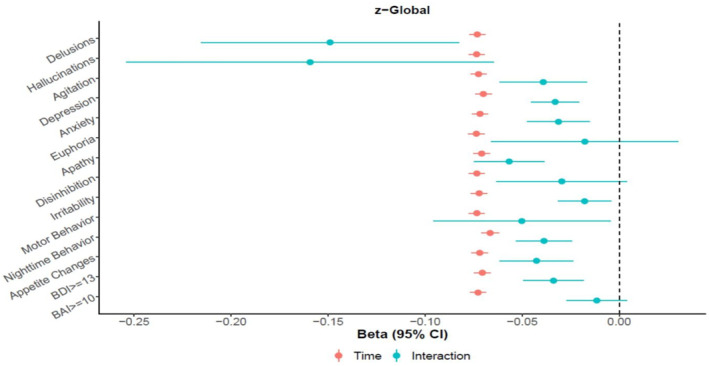
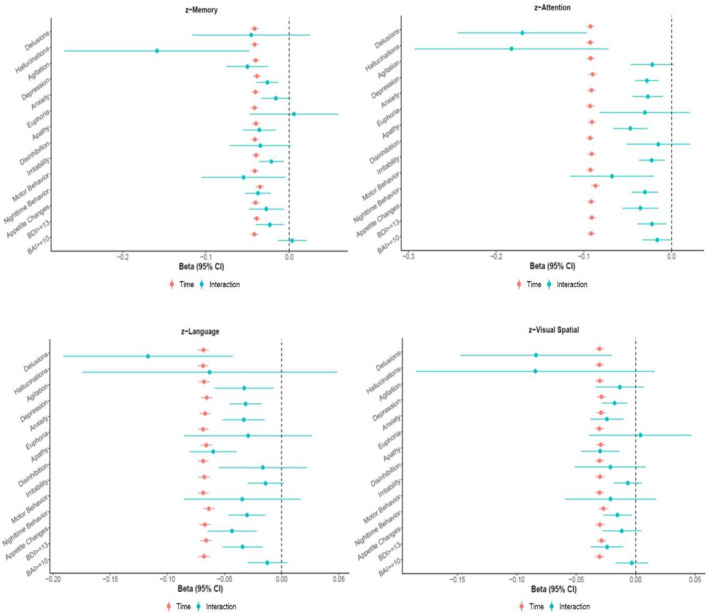
Cognition declined regardless of NPS status over the median follow-up of 4.5 years. Presence of NPS was associated with increased cognitive decline. Differences in annualized change in global cognition z-scores for participants with NPS compared to without NPS ranged from -0.018 (95% CI -0.032, -0.004; p = 0.011) for irritability to -0.159 (-0.254, -0.065; p = 0.001) for hallucinations. Associations between NPS and annual decline in global cognition were significant for most NPI-Q-assessed NPS and clinical depression (BDI-II≥13). Participants with NPI-Q-assessed depression, apathy, nighttime behavior, and clinical depression had greater decline in all domain-specific z-scores; presence of delusions and anxiety was associated with more pronounced decline in language, attention and visuospatial skills.
NPS were associated with a more accelerated cognitive decline. Clinical assessment and potential treatment of NPS is warranted even in a community setting as NPS may impact cognitive decline in nondemented individuals.
神经精神症状(NPS)与轻度认知障碍(MCI)和痴呆的发病风险相关。我们研究了 NPS 与整体和特定领域认知轨迹结果之间的关系。
在这项基于人群的梅奥诊所老龄化研究中,我们进行了一项纵向研究,纳入了 5081 名居住在社区、无痴呆的 50 岁及以上(51%为男性)个体,使用神经精神病学问卷(NPI-Q)和贝克抑郁和焦虑量表(BDI-II、BAI)评估 NPS。通过每 15 个月进行一次的神经心理学测试评估整体和特定领域(记忆、语言、注意力和视空间技能)的认知表现。使用线性混合效应模型计算基线 NPS 与个体每年认知 z 分数变化轨迹之间的关系。
无论 NPS 状态如何,认知在中位数为 4.5 年的随访期间均下降。存在 NPS 与认知下降增加相关。与无 NPS 参与者相比,有 NPS 参与者的年度全球认知 z 分数变化率差异范围为 0.018(95%CI-0.032,-0.004;p=0.011),与易激惹相关,至 0.159(95%CI-0.254,-0.065;p=0.001),与幻觉相关。与 NPS 相关的年度全球认知下降与大多数 NPI-Q 评估的 NPS 和临床抑郁(BDI-II≥13)显著相关。评估为 NPI-Q 抑郁、淡漠、夜间行为和临床抑郁的参与者,所有特定领域的 z 分数下降更大;出现妄想和焦虑与语言、注意力和视空间技能下降更显著相关。
NPS 与认知加速下降相关。即使在社区环境中,也需要对 NPS 进行临床评估和潜在治疗,因为 NPS 可能会影响非痴呆个体的认知下降。