Oh Hyun Jin, Ryu Kum Hei, Park Bum Joon, Yoon Byung-Ho
Division of Gastroenterology, Department of Internal Medicine, Center for Cancer Prevention and Detection, National Cancer Center, Goyang-si.
Department of Orthopedic Surgery, Ewha Womans University, College of Medicine, Seoul, Korea.
Medicine (Baltimore). 2021 Mar 19;100(11):e25216. doi: 10.1097/MD.0000000000025216.
Non-vitamin K antagonist oral anticoagulants (NOACs) have been widely used for stroke prevention in atrial fibrillation (AF) and the treatment and prevention of venous thromboembolism. There is an issue with safety, especially in clinically relevant bleeding. We performed a network meta-analysis to evaluate the risk of major gastrointestinal (GI) bleeding associated with NOACs.
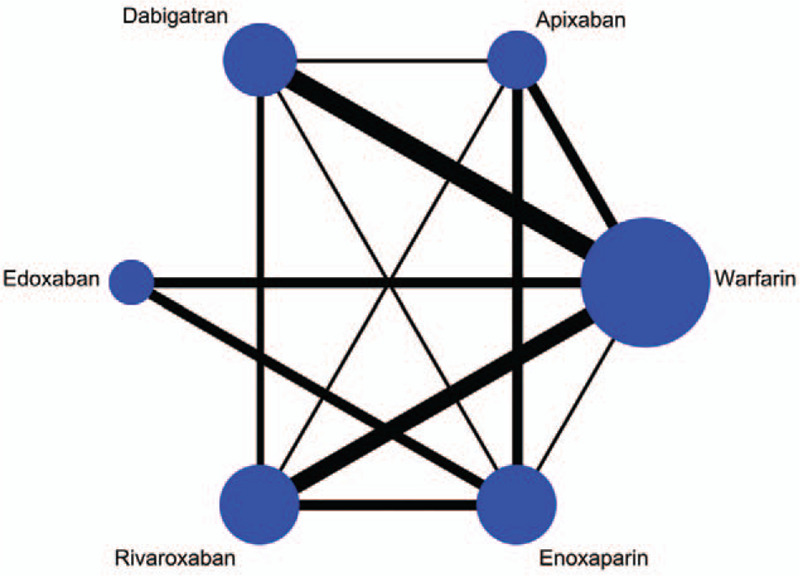
Interventions were warfarin, enoxaparin, apixaban, dabigatran, edoxaban, and rivaroxaban. The primary outcome was the incidence of major GI bleeding. A subgroup analysis was performed according to the following indications: AF, deep venous thrombosis/pulmonary embolism, and postsurgical prophylaxis.
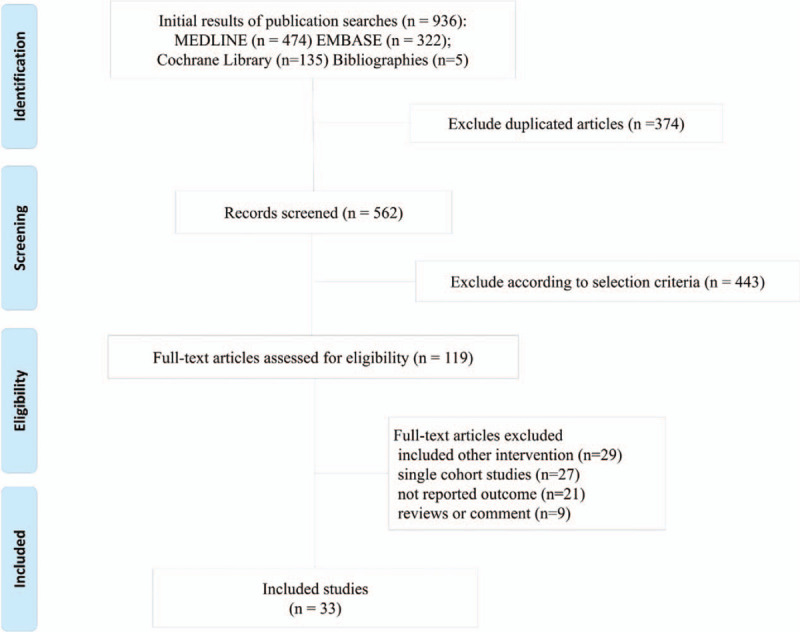
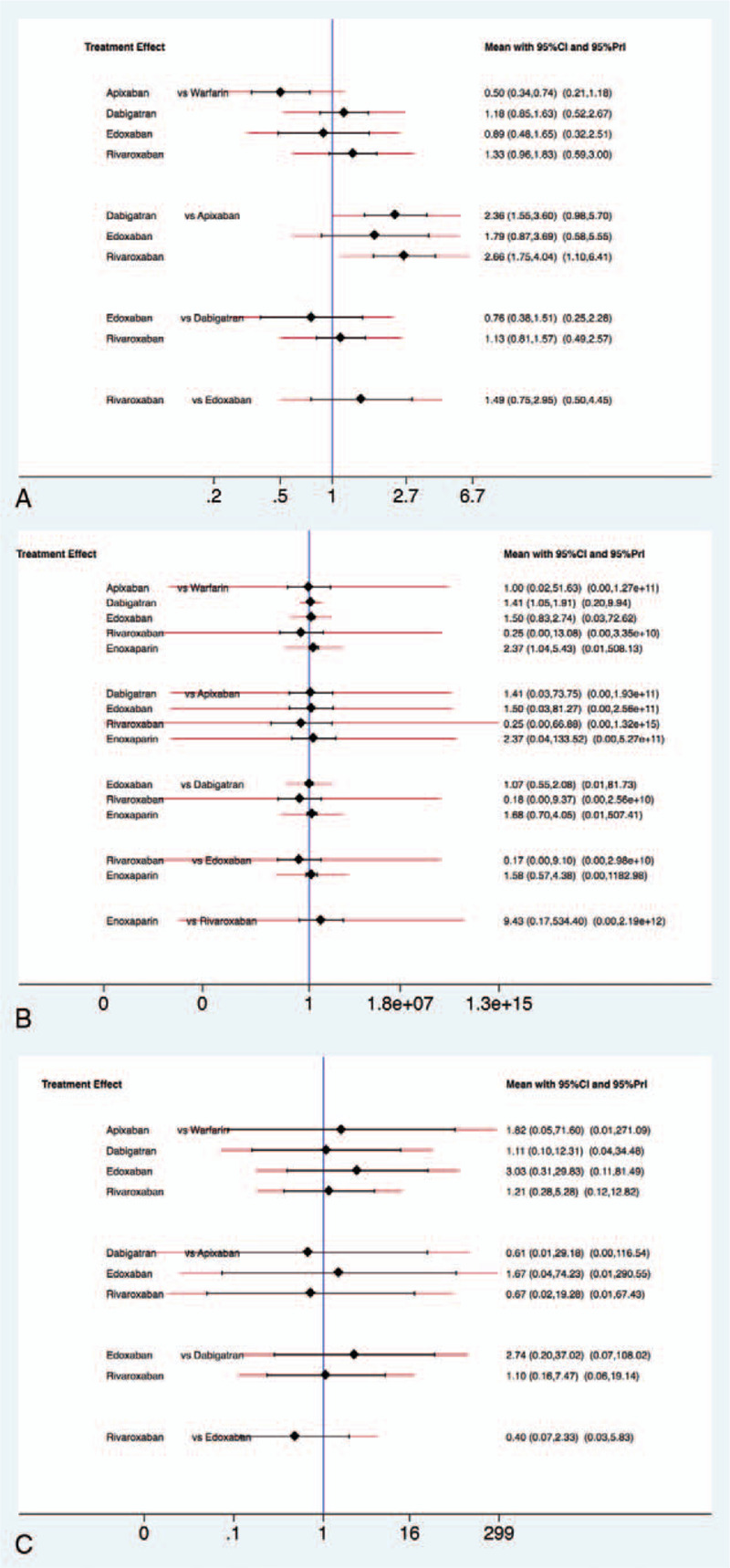
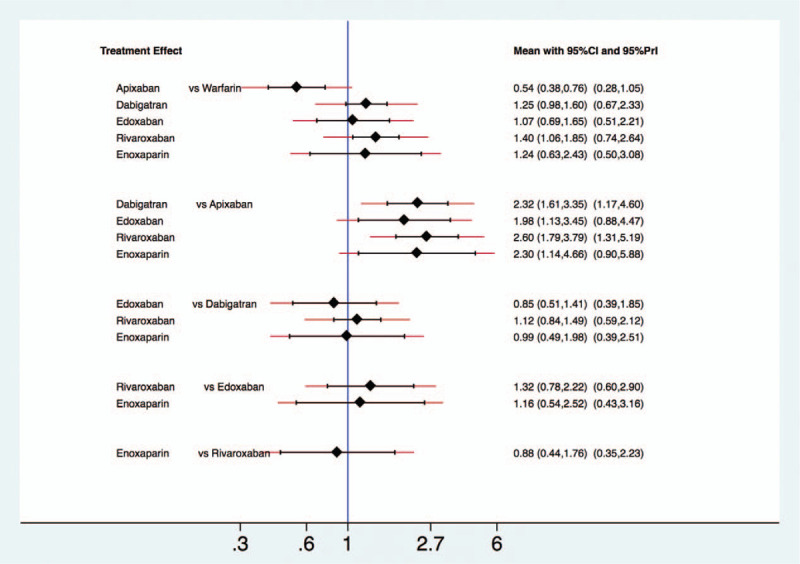
A total of 29 randomized controlled trials (RCTs) and 4 large observation population studies were included. Compared with warfarin, apixaban showed a decreased the risk of major GI bleeding (relative risk [RR] 0.54, 95% confidence interval [CI] 0.25-0.76), and rivaroxaban tended to increase this risk (RR 1.40, 95% CI 1.06-1.85). Dabigatran (RR 1.25, 95% CI 0.98-1.60), edoxaban (RR 1.07, 95% CI 0.69-1.65), and enoxaparin (RR 1.24, 95% CI 0.63-2.43) did not significantly increase the risk of GI bleeding than did warfarin. In the subgroup analysis, according to indications, apixaban showed a decreased risk of major GI bleeding (RR 0.50, 95% CI 0.34-0.74) than did warfarin in AF studies. Dabigatran (RR 2.36, 95% CI 1.55-3.60, and rivaroxaban (RR 1.75, 95% CI 1.10-6.41) increased the risk of major GI bleeding than did apixaban. An analysis of studies on venous thromboembolism or pulmonary embolism showed that no individual NOAC or enoxaparin was associated with an increased risk of major GI bleeding compared to warfarin.
Individual NOACs had varying profiles of GI bleeding risk. Results of analyses including only RCTs and those including both RCTs and population studies showed similar trends, but also showed several differences.
非维生素K拮抗剂口服抗凝药(NOACs)已广泛用于心房颤动(AF)的卒中预防以及静脉血栓栓塞的治疗和预防。存在安全性问题,尤其是在临床相关出血方面。我们进行了一项网状荟萃分析,以评估与NOACs相关的重大胃肠道(GI)出血风险。
干预措施包括华法林、依诺肝素、阿哌沙班、达比加群、依度沙班和利伐沙班。主要结局是重大GI出血的发生率。根据以下适应证进行亚组分析:AF、深静脉血栓形成/肺栓塞和术后预防。
共纳入29项随机对照试验(RCTs)和4项大型观察性人群研究。与华法林相比,阿哌沙班显示重大GI出血风险降低(相对风险[RR]0.54,95%置信区间[CI]0.25 - 0.76),而利伐沙班有增加此风险的趋势(RR 1.40,95% CI 1.06 - 1.85)。达比加群(RR 1.25,95% CI 0.98 - 1.60)、依度沙班(RR 1.07,95% CI 0.69 - 1.65)和依诺肝素(RR 1.24,95% CI 0.63 - 2.43)与华法林相比,并未显著增加GI出血风险。在亚组分析中,根据适应证,在AF研究中,阿哌沙班显示出比华法林更低的重大GI出血风险(RR 0.50,95% CI 0.34 - 0.74)。达比加群(RR 2.36,95% CI 1.55 - 3.60)和利伐沙班(RR 1.75,95% CI 1.10 - 6.41)比阿哌沙班增加了重大GI出血风险。对静脉血栓栓塞或肺栓塞研究的分析表明,与华法林相比,没有单一的NOAC或依诺肝素与重大GI出血风险增加相关。
个体NOACs的GI出血风险情况各不相同。仅包括RCTs的分析结果以及包括RCTs和人群研究的分析结果显示出相似趋势,但也存在一些差异。