Clinton Health Access Initiative, Boston, MA, USA.
Clinton Health Access Initiative, Panama City, Panama.
Glob Health Sci Pract. 2021 Mar 15;9(Suppl 1):S98-S110. doi: 10.9745/GHSP-D-20-00379.
Across the Greater Mekong Subregion (GMS) and Central America, governments commonly employ community health workers (CHWs) to improve access to and uptake of malaria services. Many of these networks are vertical in design, organized to extend malaria-only services to those remaining communities in which malaria persists.
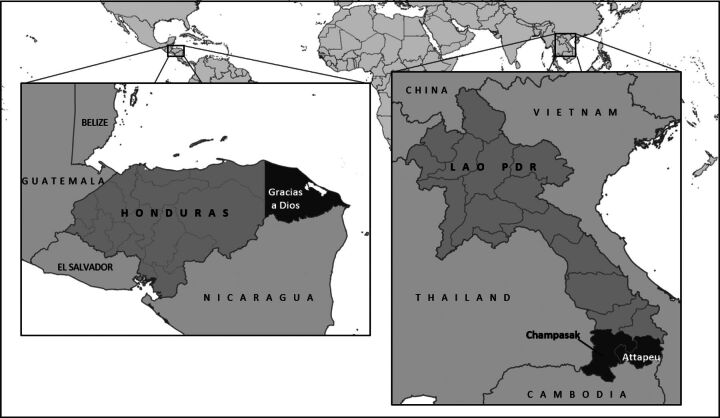
Between 2019 and 2020, national ministries of health (MOH) and Clinton Health Access Initiative conducted mixed-methods CHW program evaluations across the GMS and Central America. Routine surveillance and programmatic data were analyzed to quantify CHW contributions to malaria elimination objectives and identify gaps and challenges. Semistructured interviews were conducted with governmental and nongovernmental stakeholders from central to community level. This article draws comparisons between the Lao People's Democratic Republic (PDR) and Honduras CHW program evaluation results to distill broader hypotheses about how vertical CHW programs might evolve as their primary mission nears its end.
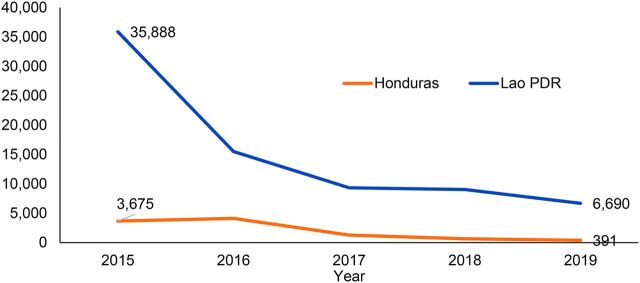
CHWs contribute substantially to malaria case detection and surveillance, diagnosing and treating 27% of malaria cases in Lao PDR and 55% in the department of Gracias a Dios, Honduras in 2019. In the same year, malaria test positivity neared less than 1% in both countries. In 2019, 80% of CHWs in Lao PDR and 74% in Gracias a Dios, Honduras did not report a single malaria case. From inception, both programs were organized as vertical (malaria-only) CHW programs reliant upon Global Fund financing for malaria commodities, training, supervision and, where applicable, remuneration.
Although community case management by CHWs has been highly impactful in reducing malaria cases to near zero, new challenges of acceptability and effectiveness of malaria-only service delivery, feasibility of continued vertical program management, and sustainable financing have emerged. To achieve and sustain reductions in malaria, surveillance and delivery platforms must be redesigned to encourage (and reward) care seeking based on experience of symptoms and not on a patient or caregiver's presumptive diagnosis of disease. By expanding the roles and responsibilities of currently vertical malaria CHWs, malarial interventions can be optimized and sustained. Such a shift will also position existing community-based platforms to be resilient and responsive as epidemiology of disease and community need shift.
在大湄公河次区域(GMS)和中美洲,各国政府通常雇用社区卫生工作者(CHW)来改善获得和接受疟疾服务的机会。这些网络中有许多是垂直设计的,旨在将仅提供疟疾服务扩展到疟疾仍然存在的那些剩余社区。
在 2019 年至 2020 年期间,各国卫生部(MOH)和克林顿健康获取倡议在 GMS 和中美洲进行了社区卫生工作者计划的混合方法评估。对常规监测和方案数据进行了分析,以量化 CHW 对消除疟疾目标的贡献,并确定差距和挑战。对从中部到社区各级的政府和非政府利益相关者进行了半结构化访谈。本文比较了老挝人民民主共和国(PDR)和洪都拉斯的 CHW 计划评估结果,以提炼出关于垂直 CHW 计划如何随着其主要任务的结束而演变的更广泛假设。
CHW 对疟疾病例的发现和监测做出了重大贡献,2019 年在老挝 PDR 诊断和治疗了 27%的疟疾病例,在洪都拉斯的 Gracias a Dios 部门诊断和治疗了 55%的疟疾病例。同年,两国的疟疾检测阳性率接近 1%。2019 年,老挝 PDR 的 80%的 CHW 和 Gracias a Dios 的 74%的 CHW 报告的疟疾病例均为零。从一开始,这两个项目都是作为垂直(仅疟疾)CHW 项目组织的,依赖全球基金提供疟疾商品、培训、监督以及在适用的情况下提供薪酬。
尽管 CHW 进行的社区病例管理在将疟疾病例减少到接近零方面非常有效,但新的挑战包括可接受性和有效性的疟疾单一服务提供、继续进行垂直计划管理的可行性以及可持续性融资。为了实现和维持疟疾的减少,监测和交付平台必须重新设计,以鼓励(并奖励)根据症状而不是根据患者或护理人员对疾病的推定诊断来寻求护理。通过扩大目前垂直疟疾 CHW 的角色和责任,可以优化和维持疟疾干预措施。这种转变还将使现有的基于社区的平台具有弹性和响应能力,因为疾病的流行病学和社区的需求正在发生变化。