Department of Thoracic Surgery, Zhongshan Hospital, Fudan University, Shanghai, China.
Department of Radiotherapy, Zhongshan Hospital, Fudan University, Shanghai, China.
JAMA Surg. 2021 May 1;156(5):444-451. doi: 10.1001/jamasurg.2021.0133.
Safety and efficacy of neoadjuvant chemoradiotherapy (nCRT) vs neoadjuvant chemotherapy (nCT) for treatment of locally advanced esophageal squamous cell carcinoma (ESCC) remain uncertain given lack of high-level clinical evidence.
To compare safety and long-term survival of nCRT followed by minimally invasive esophagectomy (MIE) with that of nCT followed by MIE for patients with locally advanced ESCC.
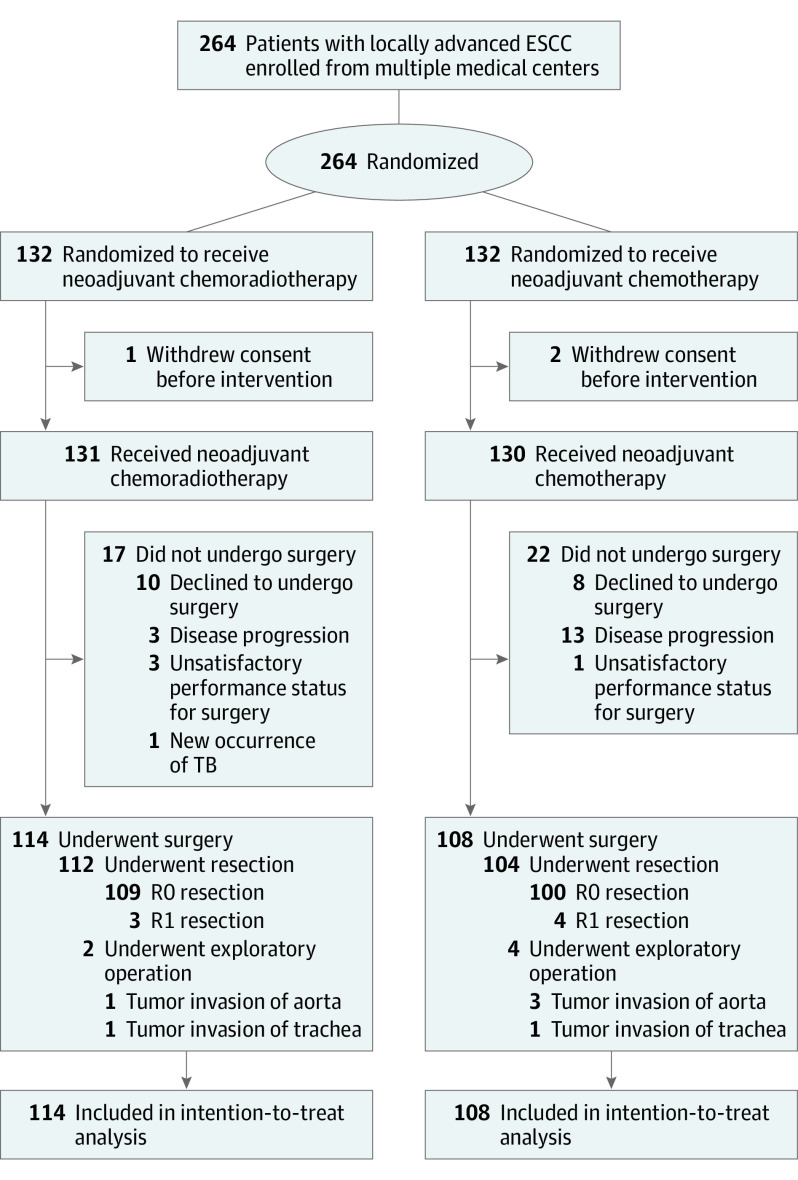
DESIGN, SETTING, AND PARTICIPANTS: A prospective, multicenter, open-label, randomized clinical trial that compared safety and efficacy of nCRT vs nCT followed by MIE for patients with locally advanced ESCC. From January 1, 2017, to December 31, 2018, 264 patients with ESCC of clinical stages from cT3 to T4aN0 to 1M0 were enrolled. Analysis was performed on an intention-to-treat basis from January 1, 2017, to August 30, 2020.
Eligible patients were randomized to the nCRT group (n = 132) or the nCT group (n = 132) by a computer-generated random system. The chemotherapy, based on paclitaxel and cisplatin, was administered to both groups, while 40 Gy of concurrent radiotherapy was added for the nCRT group. At about 6 weeks after neoadjuvant therapy, MIE via thoracoscopy and laparoscopy was performed for the patients in both groups.
The primary outcome was 3-year overall survival. Secondary outcomes included postoperative complications, mortality, postoperative pathologic outcome, recurrence-free survival time, and quality of life.
Among 264 patients (226 men [85.6%]; mean [SD] age, 61.4 [6.8] years), postoperative morbidity was 47.4% in the nCRT group (54 of 114) and 42.6% in the nCT group (46 of 108), with no significant difference between groups (difference, 4.8%; 95% CI, -8.2% to 17.5%; P = .48). Distribution of the severity of complications was similar between the 2 groups based on Clavien-Dindo classification. The 90-day perioperative mortality rate was 3.5% for the nCRT group (4 of 114) and 2.8% for the nCT group (3 of 108) (P = .94). The R0 resection rates were similar between groups (109 of 112 [97.3%] vs 100 of 104 [96.2%]; P = .92). However, patients in the nCRT group had a higher pathologic complete response (residual tumor, 0%) rate (40 of 112 [35.7%] vs 4 of 104 [3.8%]; P < .001) and a higher rate of negative lymph nodes (ypN0, 74 of 112 [66.1%] vs 48 of 104 [46.2%]; P = .03) than those in the nCT group. One-year overall survival using intention-to-treat analysis was 87.1% in the nCRT group (115 of 132) and 82.6% in the nCT group (109 of 132) (P = .30). Furthermore, deaths caused by tumor progression or recurrence were significantly less in the nCRT group than in the nCT group (9 of 132 [6.8%] vs 19 of 132 [14.4%]; P = .046); however, deaths from nontumor causes were similar (8 of 132 [6.1%] vs 4 of 132 [3.0%]; P = .24).
Initial results of the trial showed that nCRT followed by MIE has similar safety to and better histopathologic outcome than nCT followed by MIE for treatment of locally advanced ESCC.
ClinicalTrials.gov Identifier: NCT03001596.
由于缺乏高级别的临床证据,新辅助放化疗(nCRT)与新辅助化疗(nCT)治疗局部晚期食管鳞状细胞癌(ESCC)的安全性和疗效仍不确定。
比较新辅助 CRT 后微创食管切除术(MIE)与 nCT 后 MIE 治疗局部晚期 ESCC 患者的安全性和长期生存情况。
设计、地点和参与者:这是一项前瞻性、多中心、开放性、随机临床试验,比较了 nCRT 与 nCT 后 MIE 治疗局部晚期 ESCC 患者的安全性和疗效。从 2017 年 1 月 1 日至 2018 年 12 月 31 日,264 例临床分期为 cT3 至 T4aN0 至 1M0 的 ESCC 患者入组。从 2017 年 1 月 1 日至 2020 年 8 月 30 日,根据意向治疗原则进行分析。
合格患者通过计算机生成的随机系统被随机分配到 nCRT 组(n=132)或 nCT 组(n=132)。两组均接受基于紫杉醇和顺铂的化疗,同时 nCRT 组加用 40 Gy 同步放疗。新辅助治疗约 6 周后,两组患者均行胸腔镜和腹腔镜下 MIE。
主要结局是 3 年总生存率。次要结局包括术后并发症、死亡率、术后病理结果、无复发生存时间和生活质量。
在 264 例患者(226 例男性[85.6%];平均[标准差]年龄 61.4[6.8]岁)中,nCRT 组术后并发症发生率为 47.4%(114 例中的 54 例),nCT 组为 42.6%(108 例中的 46 例),两组间差异无统计学意义(差异 4.8%;95%CI-8.2%至 17.5%;P=0.48)。根据 Clavien-Dindo 分类,两组并发症严重程度分布相似。nCRT 组 90 天围手术期死亡率为 3.5%(114 例中的 4 例),nCT 组为 2.8%(108 例中的 3 例)(P=0.94)。两组 R0 切除率相似(nCRT 组 109 例[97.3%],nCT 组 100 例[96.2%];P=0.92)。然而,nCRT 组的病理完全缓解(残留肿瘤为 0%)率(40 例[35.7%])高于 nCT 组(4 例[3.8%];P<0.001),y pN0 率(112 例中 74 例[66.1%])高于 nCT 组(104 例中 48 例[46.2%];P=0.03)。意向治疗分析的 1 年总生存率在 nCRT 组为 87.1%(132 例中的 115 例),nCT 组为 82.6%(132 例中的 109 例)(P=0.30)。此外,nCRT 组肿瘤进展或复发导致的死亡明显少于 nCT 组(nCRT 组 9 例[6.8%],nCT 组 19 例[14.4%];P=0.046),但因非肿瘤原因导致的死亡相似(nCRT 组 8 例[6.1%],nCT 组 4 例[3.0%];P=0.24)。
试验的初步结果显示,新辅助 CRT 后 MIE 的安全性与 nCT 后 MIE 相似,但新辅助 CRT 后 MIE 的组织病理学疗效优于 nCT 后 MIE,可用于治疗局部晚期 ESCC。
ClinicalTrials.gov 标识符:NCT03001596。