Department of Anaesthesiology and Pain Medicine, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse, 3010, Bern, Switzerland.
Department of Anaesthesiology, Cantonal Hospital of Graubünden, Chur, Switzerland.
Scand J Trauma Resusc Emerg Med. 2021 Mar 17;29(1):49. doi: 10.1186/s13049-021-00863-9.
Tracheal intubation remains the gold standard of airway management in emergency medicine and maximizing safety, intubation success, and especially first-pass intubation success (FPS) in these situations is imperative.
We conducted a prospective observational study on all 12 helicopter emergency medical service (HEMS) bases of the Swiss Air Rescue, between February 15, 2018, and February 14, 2019. All 428 patients on whom out-of-hospital advanced airway management was performed by the HEMS crew were included. The C-MAC video laryngoscope was used as the primary device for tracheal intubation. Intubation procedures were recorded by the video laryngoscope and precise time points were recorded to verify the time necessary for each attempt and the overall procedure time until successful intubation. The videos were further analysed for problems and complications during airway management by an independent reviewer. Additionally, a questionnaire about the intubation procedure, basic characteristics of the patient, circumstances, environmental factors, and the provider's level of experience in airway management was filled out. Main outcome measures were FPS of tracheal intubation, overall success rate, overall intubation time, problems and complications of video laryngoscopy.
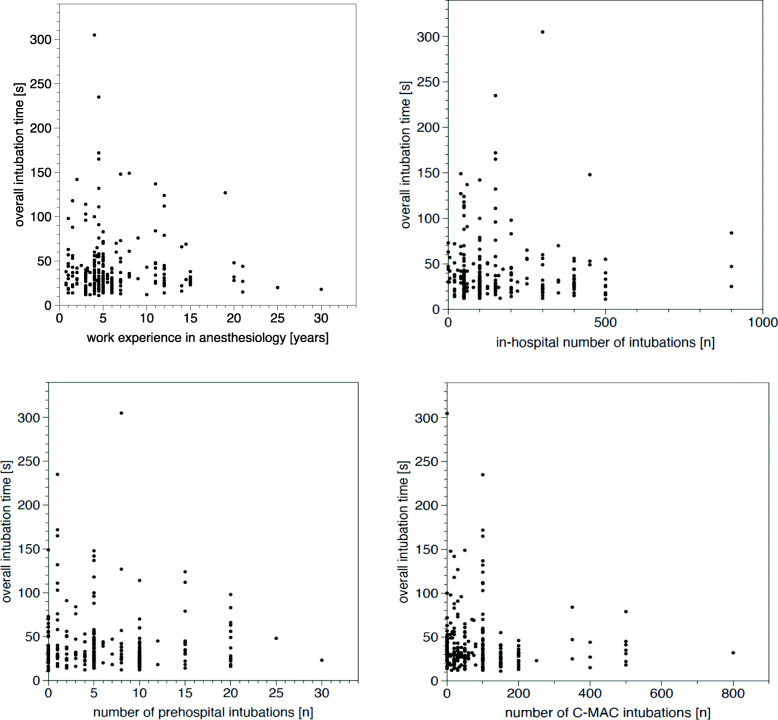
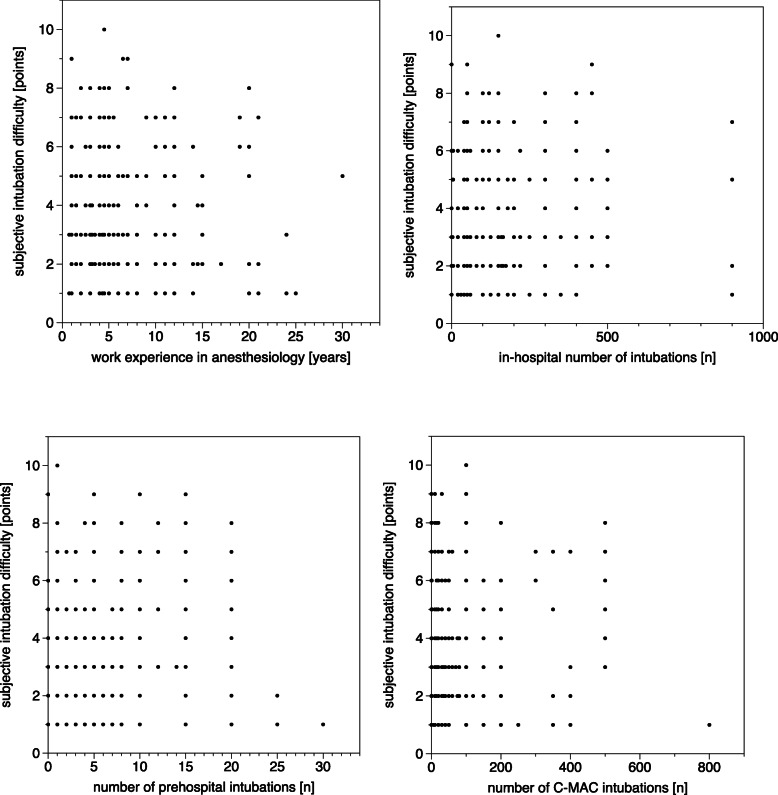
FPS rate was 87.6% and overall success rate 98.6%. Success rates, overall time to intubation, and subjective difficulty were not associated to the providers' expertise in airway management. In patients undergoing CPR FPS was 84.8%, in trauma patients 86.4% and in non-trauma patients 93.3%. FPS in patients with difficult airway characteristics, facial trauma/burns or obesity ranges between 87 and 89%. Performing airway management indoors or inside an ambulance resulted in a significantly higher FPS of 91.1% compared to outdoor locations (p < 0.001). Direct solar irradiation on the screen, fogging of the lens, and blood on the camera significantly impaired FPS. Several issues for further improvements in the use of video laryngoscopy in the out-of-hospital setting and for quality control in airway management were identified.
Airway management using the C-MAC video laryngoscope with Macintosh blade in a group of operators with mixed experience showed high FPS and overall rates of intubation success. Video recording emergency intubations may improve education and quality control.
气管插管仍然是急诊医学中气道管理的金标准,最大限度地提高安全性、插管成功率,尤其是首次插管成功率(FPS)至关重要。
我们对瑞士空中救援的所有 12 个直升机紧急医疗服务(HEMS)基地进行了一项前瞻性观察研究,时间为 2018 年 2 月 15 日至 2019 年 2 月 14 日。所有在 HEMS 机组人员进行院外高级气道管理的 428 名患者均被纳入研究。C-MAC 视频喉镜被用作气管插管的主要设备。插管过程由视频喉镜记录,并记录精确的时间点以验证每次尝试所需的时间以及直至成功插管的总程序时间。由一名独立审查员对气道管理过程中的问题和并发症进行进一步分析。此外,还填写了一份关于插管程序、患者基本特征、情况、环境因素以及提供者气道管理经验水平的问卷。主要观察指标为气管插管的 FPS、总体成功率、总体插管时间、视频喉镜的问题和并发症。
FPS 率为 87.6%,总体成功率为 98.6%。成功率、插管总时间以及主观难度与提供者的气道管理专业知识无关。在接受心肺复苏(CPR)的患者中,FPS 为 84.8%,在创伤患者中为 86.4%,在非创伤患者中为 93.3%。在具有困难气道特征、面部创伤/烧伤或肥胖的患者中,FPS 范围在 87%至 89%之间。在室内或救护车内部进行气道管理的 FPS 显著高于户外(p<0.001)。阳光直射屏幕、镜头起雾和摄像头有血会显著降低 FPS。确定了一些在院外环境中进一步改进视频喉镜使用和气道管理质量控制的问题。
在一组经验混合的操作人员中,使用 C-MAC 视频喉镜和 Macintosh 叶片进行气道管理可实现高 FPS 和总体插管成功率。对紧急插管进行视频记录可能会改善教育和质量控制。