Department of Clinical Neurosciences and Cambridge University Hospitals NHS Trust, University of Cambridge, Cambridge, UK.
Institute of Molecular Bioimaging and Physiology, National Research Council, Milan, Italy.
J Neurol Neurosurg Psychiatry. 2021 Jul;92(7):769-775. doi: 10.1136/jnnp-2020-325549. Epub 2021 Mar 17.
In addition to tau pathology and neuronal loss, neuroinflammation occurs in progressive supranuclear palsy (PSP). However, the prognostic value of the in vivo imaging markers for these processes in PSP remains unclear. We test the primary hypothesis that baseline in vivo imaging assessment of neuroinflammation in subcortical regions predicts clinical progression in patients with PSP.
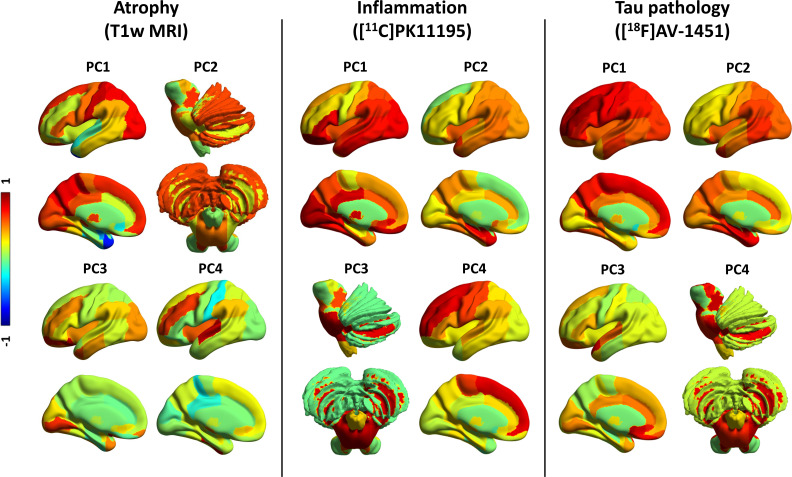
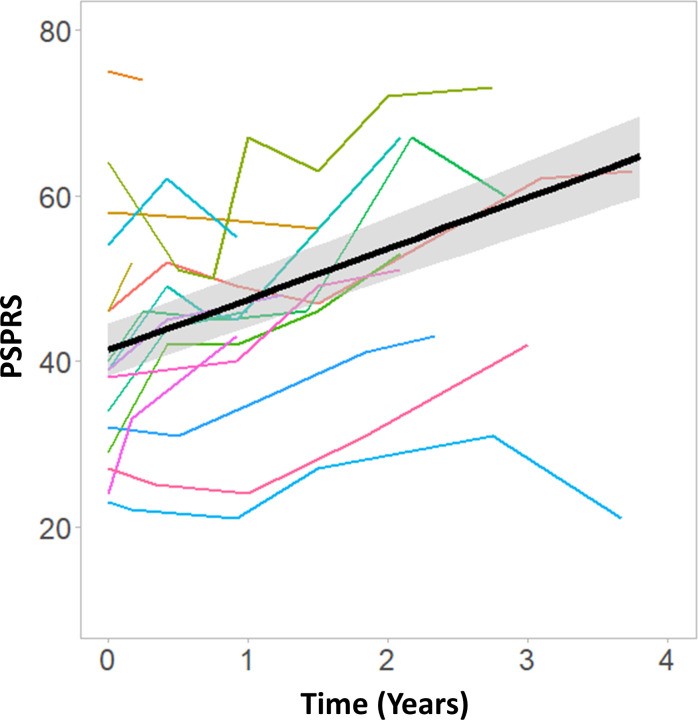
Seventeen patients with PSP-Richardson's syndrome underwent a baseline multimodal imaging assessment, including [C]PK11195 positron emission tomography (PET) to index microglial activation, [F]AV-1451 PET for tau pathology and structural MRI. Disease severity was measured at baseline and serially up to 4 years with the Progressive Supranuclear Palsy Rating Scale (PSPRS) (average interval of 5 months). Regional grey-matter volumes and PET ligand binding potentials were summarised by three principal component analyses (PCAs). A linear mixed-effects model was applied to the longitudinal PSPRS scores. Single-modality imaging predictors were regressed against the individuals' estimated rate of progression to identify the prognostic value of baseline imaging markers.
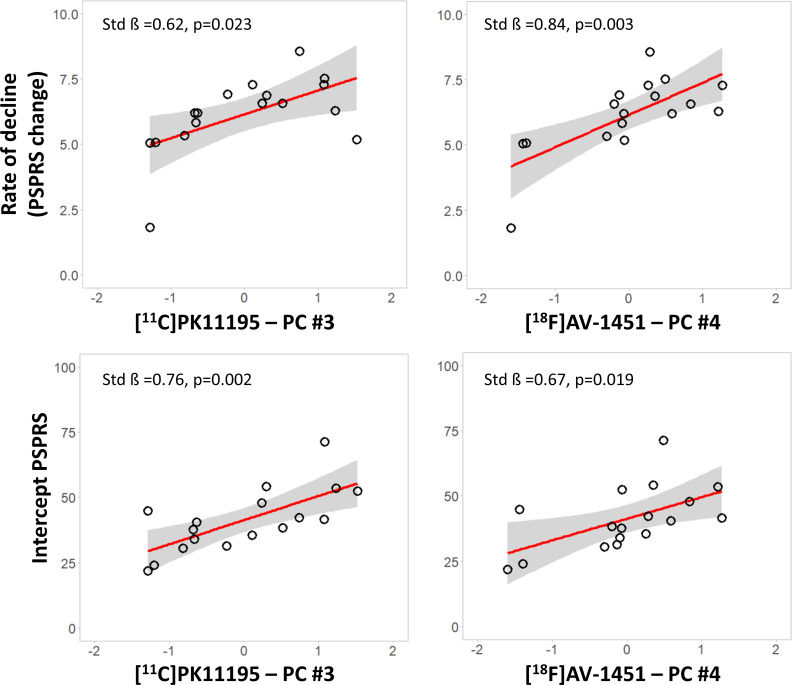
PCA components reflecting neuroinflammation and tau burden in the brainstem and cerebellum correlated with the subsequent annual rate of change in the PSPRS. PCA-derived PET markers of neuroinflammation and tau pathology correlated with regional brain volume in the same regions. However, MRI volumes alone did not predict the rate of clinical progression.
Molecular imaging with PET for microglial activation and tau pathology can predict clinical progression in PSP. These data encourage the evaluation of immunomodulatory approaches to disease-modifying therapies in PSP and the potential for PET to stratify patients in early phase clinical trials.
除了 tau 病理学和神经元丢失外,神经炎症也发生在进行性核上性麻痹(PSP)中。然而,这些过程的体内成像标志物在 PSP 中的预后价值尚不清楚。我们检验了一个主要假设,即亚皮质区域的神经炎症的基线体内成像评估可预测 PSP 患者的临床进展。
17 名 PSP-Richardson 综合征患者接受了基线多模态成像评估,包括[C]PK11195 正电子发射断层扫描(PET)以评估小胶质细胞激活、[F]AV-1451 PET 以评估 tau 病理学和结构 MRI。使用进行性核上性麻痹评分量表(PSPRS)(平均间隔 5 个月)在基线和连续 4 年内测量疾病严重程度。通过三个主成分分析(PCA)总结了区域灰质体积和 PET 配体结合潜力。线性混合效应模型应用于纵向 PSPRS 评分。将单模态成像预测因子回归到个体的估计进展率,以确定基线成像标志物的预后价值。
反映脑桥和小脑神经炎症和 tau 负担的 PCA 成分与 PSPRS 的后续年度变化率相关。脑内神经炎症和 tau 病理学的 PCA 衍生 PET 标志物与同一区域的脑体积相关。然而,MRI 体积本身并不能预测临床进展的速度。
使用 PET 进行的小胶质细胞激活和 tau 病理学的分子成像可以预测 PSP 的临床进展。这些数据鼓励在 PSP 中评估针对疾病修饰疗法的免疫调节方法,以及 PET 对早期临床试验中患者进行分层的潜力。