Wei Shijun, Fan Dongsheng, Han Fang, Tang Ming, Kong Changwang, Xu Feng, Cai Xianhua
Department of Orthopaedics, General Hospital of Central Theater Command (Wuhan General Hospital of Guangzhou Command, previously), NO. 627, Wuluo Road, Wuhan, 430030, Hubei Province, People's Republic of China.
The First Clinical Medical School of Southern Medical University, Guangzhou, Guangdong Province, People's Republic of China.
BMC Musculoskelet Disord. 2021 Mar 18;22(1):289. doi: 10.1186/s12891-021-04165-0.
Minimally invasive reconstruction techniques are used for anatomical ligament construction of the lateral collateral ligament complex of the ankle, but the two key elements, the bone tunnel and the appropriate graft tension, for the identification of the anatomic location during the surgery are not clearly stated.
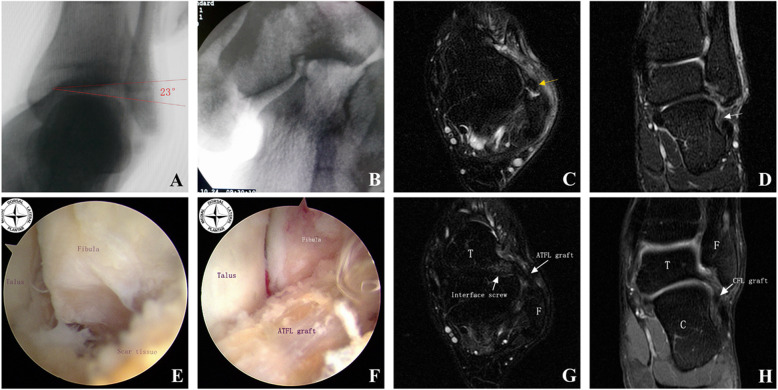
The patients with chronic ankle instability who received arthroscopic anatomic lateral ligament complex reconstruction were retrospectively analyzed. The anatomical location of the bone tunnel was performed under arthroscopy combined with fluoroscopy for accurate location of the bone tunnel entrance. The graft tension and routing were controlled under arthroscopic visualization. The clinical outcomes were assessed using the Karlsson-Peterson score, Sefton articular stability scale, and Visual Analogue Scale (VAS). The complications were recorded during the follow-up.
A total of 18 patients were enrolled in this study. The mean follow-up was 33.33 ± 3.69 (range from 24 to 36) months. No patient had recurrence of ankle instability after the operation. According to the Sefton articular stability scale, 94.5% of the patients had excellent/good function. The mean value of the anterior drawer tests and the talar tilt angle examination were decreased. The mean of the Karlsson-Peterson score and the Visual Analogue Scale(VAS) score were both improved significantly.
The anatomic reconstruction of the ankle lateral ligament complex to treat chronic ankle instability using the arthroscopy combined with the fluoroscopic technique could improve the clinical functions, satisfaction, and reduced pain of patients.
微创重建技术用于踝关节外侧副韧带复合体的解剖学韧带构建,但手术过程中用于确定解剖位置的两个关键要素,即骨隧道和合适的移植物张力,并未明确说明。
对接受关节镜下解剖学外侧韧带复合体重建的慢性踝关节不稳患者进行回顾性分析。在关节镜联合透视下确定骨隧道的解剖位置,以精确确定骨隧道入口。在关节镜直视下控制移植物的张力和走行。使用卡尔森-彼得森评分、塞夫顿关节稳定性量表和视觉模拟量表(VAS)评估临床结果。随访期间记录并发症情况。
本研究共纳入18例患者。平均随访时间为33.33 ± 3.69(24至36)个月。术后无患者出现踝关节不稳复发。根据塞夫顿关节稳定性量表,94.5%的患者功能为优/良。前抽屉试验和距骨倾斜角检查的平均值降低。卡尔森-彼得森评分和视觉模拟量表(VAS)评分的平均值均显著提高。
采用关节镜联合透视技术对踝关节外侧韧带复合体进行解剖重建以治疗慢性踝关节不稳,可改善患者的临床功能、满意度并减轻疼痛。