Department of Orthopaedic Surgery, Academic Medical Centre, Amsterdam Movement Sciences, University of Amsterdam, PO Box 22660, 1100 DD, Amsterdam, The Netherlands.
Academic Center for Evidence Based Sports Medicine (ACES), Amsterdam, The Netherlands.
Knee Surg Sports Traumatol Arthrosc. 2018 Jul;26(7):2183-2195. doi: 10.1007/s00167-017-4730-4. Epub 2017 Nov 14.
To determine the best surgical treatment for chronic ankle instability (CAI) a systematic review was performed to compare the functional outcomes between various surgical stabilization methods.
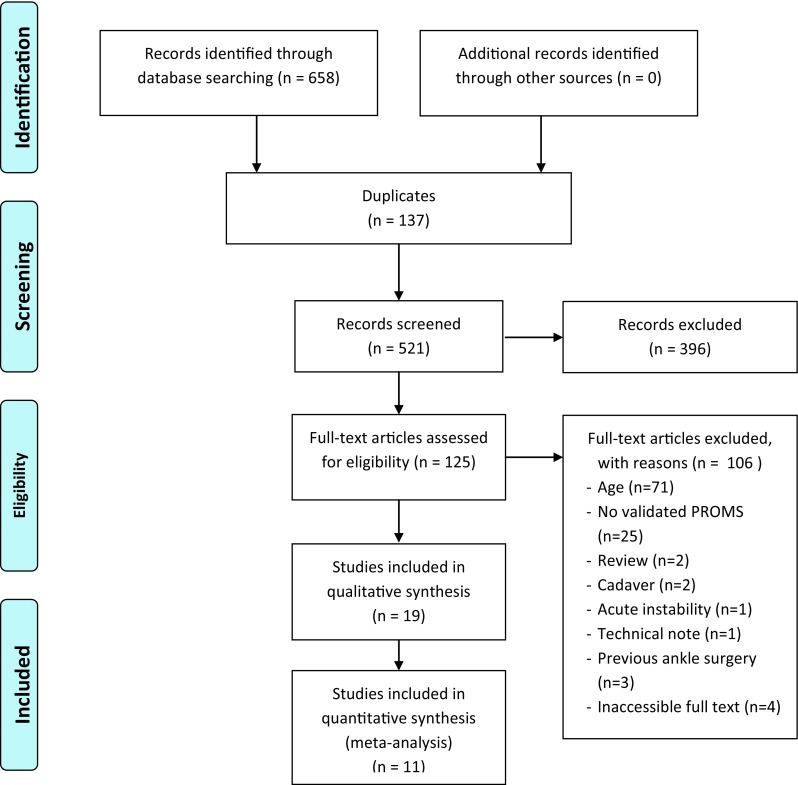
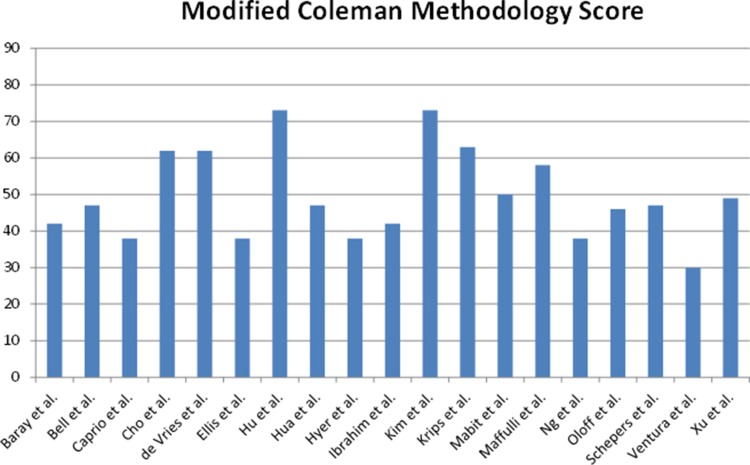
A systematic search was performed from 1950 up to April 2016 using PubMed, EMBASE, Medline and the Cochrane Library. Inclusion criteria were a minimum age of 18 years, persistent lateral ankle instability, treatment by some form of surgical stabilization, described functional outcome measures. Exclusion criteria were case reports, (systematic) reviews, articles not published in English, description of only acute instability or only conservative treatment, medial ankle instability and concomitant injuries, deformities or previous surgical treatment for ankle instability. After inclusion, studies were critically appraised using the Modified Coleman Methodology Score.
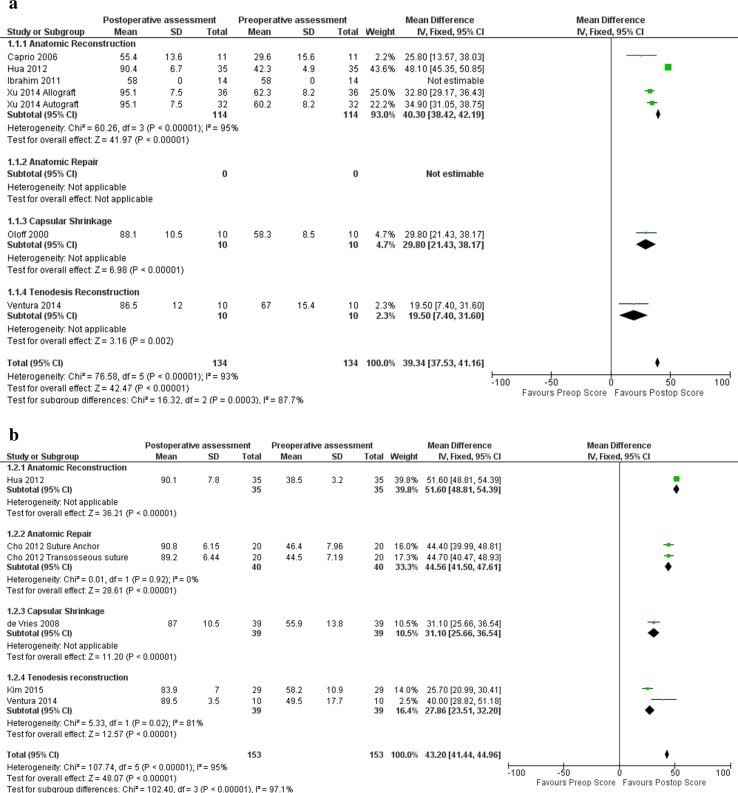
The search resulted in a total of 19 articles, including 882 patients, which were included in this review. The Modified Coleman Methodology Score ranged from 30 to 73 points on a scale from 0 to 90 points. The AOFAS and Karlsson Score were the most commonly used patient-reported outcome measures to assess functional outcome after surgery. Anatomic repair showed the highest post-operative scores [AOFAS 93.8 (SD ± 2.7; n = 119); Karlsson 95.1 (SD ± 3.6, n = 121)], compared to anatomic reconstruction [AOFAS 90.2 (SD ± 10.9, n = 128); Karlsson 90.1 (SD ± 7.8, n = 35)] and tenodesis [AOFAS 86.5 (SD ± 12.0, n = 10); Karlsson 85.3 (SD ± 2.5, n = 39)]. Anatomic reconstruction showed the highest score increase after surgery (AOFAS 37.0 (SD ± 6.8, n = 128); Karlsson 51.6 (SD ± 5.5, n = 35) compared to anatomic repair [AOFAS 31.8 (SD ± 5.3, n = 119); Karlsson 40.9 (SD ± 2.9, n = 121)] and tenodesis [AOFAS 19.5 (SD ± 13.7, n = 10); Karlsson 29.4 (SD ± 6.3, n = 39)] (p < 0.005).
Anatomic reconstruction and anatomic repair provide better functional outcome after surgical treatment of patients with CAI compared to tenodesis reconstruction. These results further discourage the use of tenodesis reconstruction and other non-anatomic surgical techniques. Future studies may be required to indicate potential value of tenodesis reconstruction when used as a salvage procedure. Not optimal, but the latter still provides an increase in functional outcome post-operatively. Anatomic reconstruction seems to give the best results, but may be more invasive than anatomic repair. This has to be kept in mind when choosing between reconstruction and repair in the treatment of CAI.
IV.
为了确定慢性踝关节不稳定(CAI)的最佳手术治疗方法,我们进行了一项系统评价,以比较各种手术稳定方法的功能结果。
从 1950 年到 2016 年 4 月,使用 PubMed、EMBASE、Medline 和 Cochrane 图书馆进行了系统搜索。纳入标准为年龄至少 18 岁,持续的外侧踝关节不稳定,接受某种形式的手术稳定治疗,描述功能结果测量。排除标准为病例报告、(系统)综述、未以英文发表的文章、仅描述急性不稳定或仅保守治疗、内侧踝关节不稳定和伴随损伤、畸形或以前的踝关节不稳定手术治疗。纳入后,使用改良 Coleman 方法学评分对研究进行严格评估。
搜索共产生 19 篇文章,包括 882 例患者,这些患者被纳入本综述。改良 Coleman 方法学评分范围为 0 至 90 分,从 30 至 73 分。AOFAS 和 Karlsson 评分是最常用于评估手术后功能结果的患者报告结局测量。解剖修复术后评分最高[AOFAS 93.8(SD ± 2.7;n = 119);Karlsson 95.1(SD ± 3.6,n = 121)],与解剖重建[AOFAS 90.2(SD ± 10.9,n = 128);Karlsson 90.1(SD ± 7.8,n = 35)]和肌腱固定[AOFAS 86.5(SD ± 12.0,n = 10);Karlsson 85.3(SD ± 2.5,n = 39)]相比。解剖重建术后评分增加最高(AOFAS 37.0(SD ± 6.8,n = 128);Karlsson 51.6(SD ± 5.5,n = 35),与解剖修复[AOFAS 31.8(SD ± 5.3,n = 119);Karlsson 40.9(SD ± 2.9,n = 121)]和肌腱固定[AOFAS 19.5(SD ± 13.7,n = 10);Karlsson 29.4(SD ± 6.3,n = 39)]相比(p < 0.005)。
与肌腱固定重建相比,解剖重建和解剖修复可为 CAI 患者的手术治疗提供更好的功能结果。这些结果进一步阻止了肌腱固定重建和其他非解剖手术技术的使用。可能需要进一步的研究来表明肌腱固定重建在作为挽救性手术时的潜在价值。虽然不是最佳选择,但后者仍能在术后提供功能结果的提高。解剖重建似乎效果最好,但可能比解剖修复更具侵袭性。在 CAI 的治疗中,选择重建还是修复时需要考虑到这一点。
IV。