Hong Jin, Tong Yiwei, He Jianrong, Chen Xiaosong, Shen Kunwei
Department of General Surgery, Comprehensive Breast Health Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Comprehensive Breast Health Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, 197 Ruijin Er Road, Shanghai 200025, China.
Ther Adv Med Oncol. 2021 Feb 26;13:1758835921996673. doi: 10.1177/1758835921996673. eCollection 2021.
Axillary node status is used in clinical practice to guide the selection of axillary surgery in breast cancer patients. However, to date, the optimal axillary management following neoadjuvant therapy (NAT) for breast cancer remains controversial. Our study aimed to investigate the association of molecular subtype, clinical stage, and ypN status after NAT in breast cancer patients, especially those achieving breast pathological complete remission (pCR).
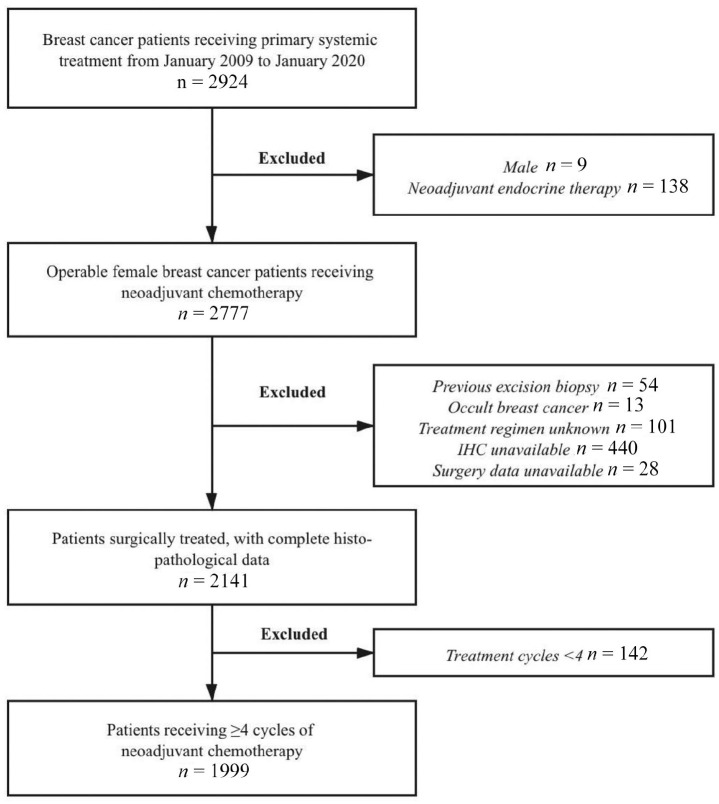
Patients receiving ⩾4 cycles of NAT were retrospectively included between January 2009 and January 2020. ypN status was compared among patients with different breast pCR statuses, clinical stages, and molecular subtypes in univariate and multivariate analyses.
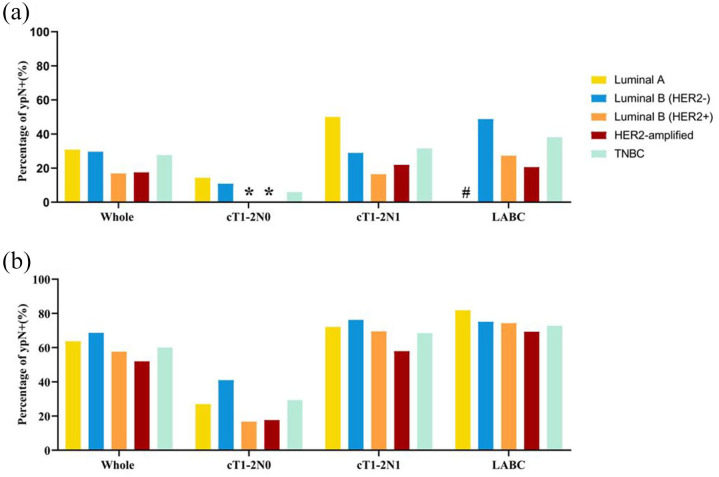
A total of 1999 patients were included: 457 (22.86%), 884 (44.22%), and 658 (32.92%) patients with cT1-2N0, cT1-2N1, and locally advanced breast cancer (LABC), respectively. Altogether, 435 (21.8%) patients achieved breast pCR: 331 with ypN- and 104 with ypN+ status. Patients achieving breast pCR had a significantly lower ypN+ rate than those without pCR [23.9% 62.5%, odds ratio (OR) = 0.14, 95% confidence interval (CI) = 0.09-0.21]. For patients with breast pCR, the ypN+ rate was 6.4%, 25.7%, and 33.9% in cT1-2N0, cT1-2N1, and LABC patients, respectively ( < 0.001). Furthermore, the ypN+ rate was 30.8%, 16.8%, 17.5%, 29.6%, and 27.6% in breast pCR patients with the Luminal A, Luminal B (HER2+), HER2-amplified, Luminal B (HER2-), and triple-negative subtype, respectively. Luminal B (HER2+) (OR = 0.20, 95% CI = 0.05-0.82) and HER2-amplified (OR = 0.19, 95% CI = 0.05-0.83) tumors were associated with lower ypN+ rates. Moreover, 100% of breast pCR patients with cT1-2N0 and HER2-positive disease achieved pathological pN0.
In breast pCR patients after NAT, clinical stage and molecular subtype were significantly associated with ypN status. Patients with cT1-2N0 and HER2-positive disease who achieved breast pCR had a very low ypN+ rate, possibly indicating the possibility for de-escalation of axillary surgery in this patient subgroup.
腋窝淋巴结状态在临床实践中用于指导乳腺癌患者腋窝手术的选择。然而,迄今为止,乳腺癌新辅助治疗(NAT)后的最佳腋窝管理仍存在争议。我们的研究旨在调查乳腺癌患者NAT后的分子亚型、临床分期和ypN状态之间的关联,尤其是那些实现乳腺病理完全缓解(pCR)的患者。
回顾性纳入2009年1月至2020年1月期间接受≥4周期NAT的患者。在单因素和多因素分析中,比较不同乳腺pCR状态、临床分期和分子亚型患者的ypN状态。
共纳入1999例患者:cT1-2N0、cT1-2N1和局部晚期乳腺癌(LABC)患者分别为457例(22.86%)、884例(44.22%)和658例(32.92%)。共有435例(21.8%)患者实现乳腺pCR:331例ypN-状态和104例ypN+状态。实现乳腺pCR的患者ypN+率显著低于未实现pCR的患者[23.9%对62.5%,比值比(OR)=0.14,95%置信区间(CI)=0.09-0.21]。对于乳腺pCR患者,cT1-2N0、cT1-2N1和LABC患者的ypN+率分别为6.4%、25.7%和33.9%(P<0.001)。此外,Luminal A、Luminal B(HER2+)、HER2扩增、Luminal B(HER2-)和三阴性亚型的乳腺pCR患者的ypN+率分别为30.8%、16.8%、17.5%、29.6%和27.6%。Luminal B(HER2+)(OR=0.20,95%CI=0.05-0.82)和HER2扩增(OR=0.19,95%CI=0.05-0.83)肿瘤与较低的ypN+率相关。此外,cT1-2N0且HER2阳性疾病的乳腺pCR患者100%实现病理pN0。
在NAT后的乳腺pCR患者中,临床分期和分子亚型与ypN状态显著相关。cT1-2N0且HER2阳性疾病且实现乳腺pCR的患者ypN+率非常低,这可能表明该患者亚组有腋窝手术降阶梯的可能性。