Department of Cardiology, Erasmus MC University Medical Center, Room Na-316, 's Gravendijkwal 230, 3015 CE, Rotterdam, The Netherlands.
Cardiovascular Research School COEUR, Erasmus MC University Medical Center, Rotterdam, The Netherlands.
J Nephrol. 2021 Oct;34(5):1421-1427. doi: 10.1007/s40620-021-01014-0. Epub 2021 Mar 18.
High mortality and rehospitalization rates demonstrate that improving risk assessment in heart failure patients remains challenging. Individual temporal evolution of kidney biomarkers is associated with poor clinical outcome in these patients and hence may carry the potential to move towards a personalized screening approach.
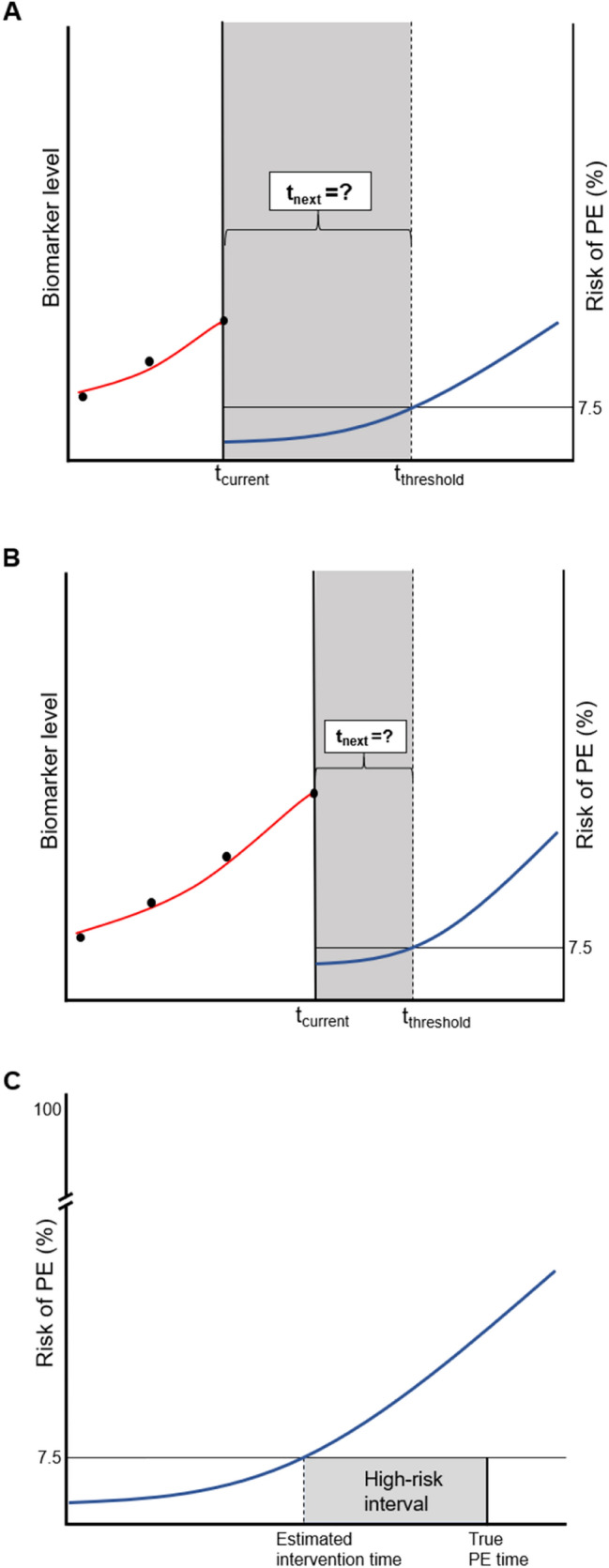
In 263 chronic heart failure patients included in the prospective Bio-SHiFT cohort study, glomerular and tubular biomarker measurements were serially obtained according to a pre-scheduled, fixed trimonthly scheme. The primary endpoint (PE) comprised cardiac death, cardiac transplantation, left ventricular assist device implantation or heart failure hospitalization. Personalized scheduling of glomerular and tubular biomarker measurements was compared to fixed scheduling in individual patients by means of a simulation study, based on clinical characteristics of the Bio-SHiFT study. For this purpose, repeated biomarker measurements and the PE were jointly modeled. For personalized scheduling, using this fitted joint model, we determined the optimal time point of the next measurement based on the patient's individual risk profile as estimated by the joint model and the maximum information gain on the patient's prognosis. We compared the schedule's capability of enabling timely intervention before the occurrence of the PE and number of measurements needed.
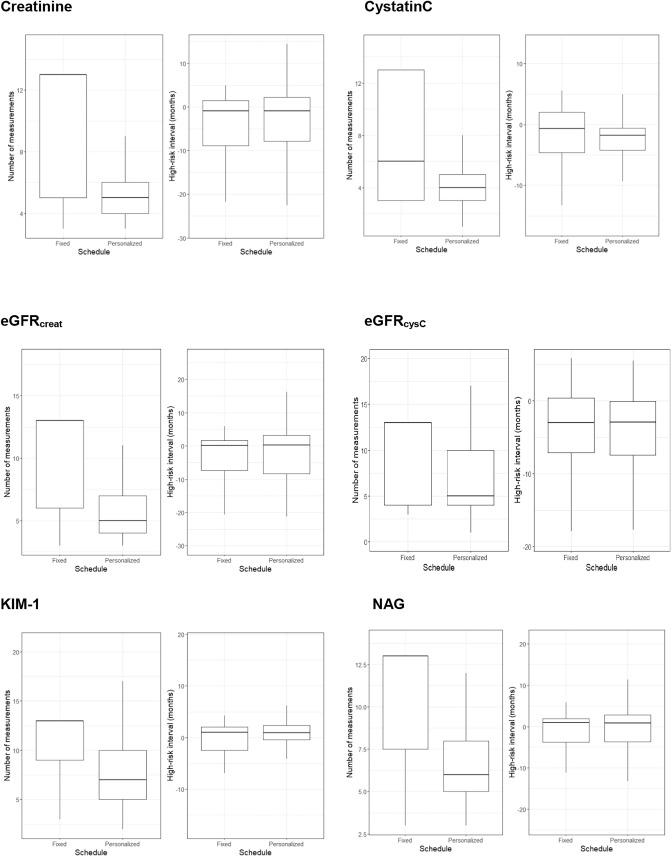
As compared to a pre-defined trimonthly scheduling approach, personalized scheduling of glomerular and tubular biomarker measurements showed similar performance with regard to prognostication, but required a median of 0.4-2.7 fewer measurements per year.
Personalized scheduling is expected to reduce the number of patient visits and healthcare costs. Thus, it may contribute to efficient monitoring of chronic heart failure patients and could provide novel opportunities for timely adaptation of treatment.
高死亡率和再住院率表明,改善心力衰竭患者的风险评估仍然具有挑战性。这些患者的肾脏生物标志物的个体时间演变与不良临床结局相关,因此可能有潜力朝着个性化筛查方法发展。
在前瞻性 Bio-SHiFT 队列研究中纳入的 263 例慢性心力衰竭患者中,根据预先设定的固定每三个月一次的方案,连续获得肾小球和肾小管生物标志物测量值。主要终点(PE)包括心脏死亡、心脏移植、左心室辅助装置植入或心力衰竭住院。通过基于 Bio-SHiFT 研究的临床特征的模拟研究,比较了个体患者中肾小球和肾小管生物标志物测量的个性化计划与固定计划。为此,使用重复的生物标志物测量值和 PE 对其进行了联合建模。对于个性化计划,我们根据联合模型估计的患者个体风险概况以及对患者预后的最大信息增益,使用该拟合联合模型确定下一次测量的最佳时间点。我们比较了该计划在发生 PE 之前及时进行干预的能力和所需的测量次数。
与预先定义的每三个月一次的计划方法相比,肾小球和肾小管生物标志物测量的个性化计划在预测方面表现相似,但每年需要的中位数测量次数减少了 0.4-2.7 次。
个性化计划有望减少患者就诊次数和医疗保健成本。因此,它可能有助于对慢性心力衰竭患者进行有效的监测,并为及时调整治疗提供新的机会。