Department of Hematology, Hemostasis, Oncology and Stem Cell Transplantation, Hannover Medical School, Carl-Neuberg-Str. 1, 30625, Hannover, Germany.
Johns Hopkins Sidney Kimmel Comprehensive Cancer Center, Baltimore, MD, USA.
Ann Hematol. 2021 May;100(5):1181-1194. doi: 10.1007/s00277-021-04465-4. Epub 2021 Mar 19.
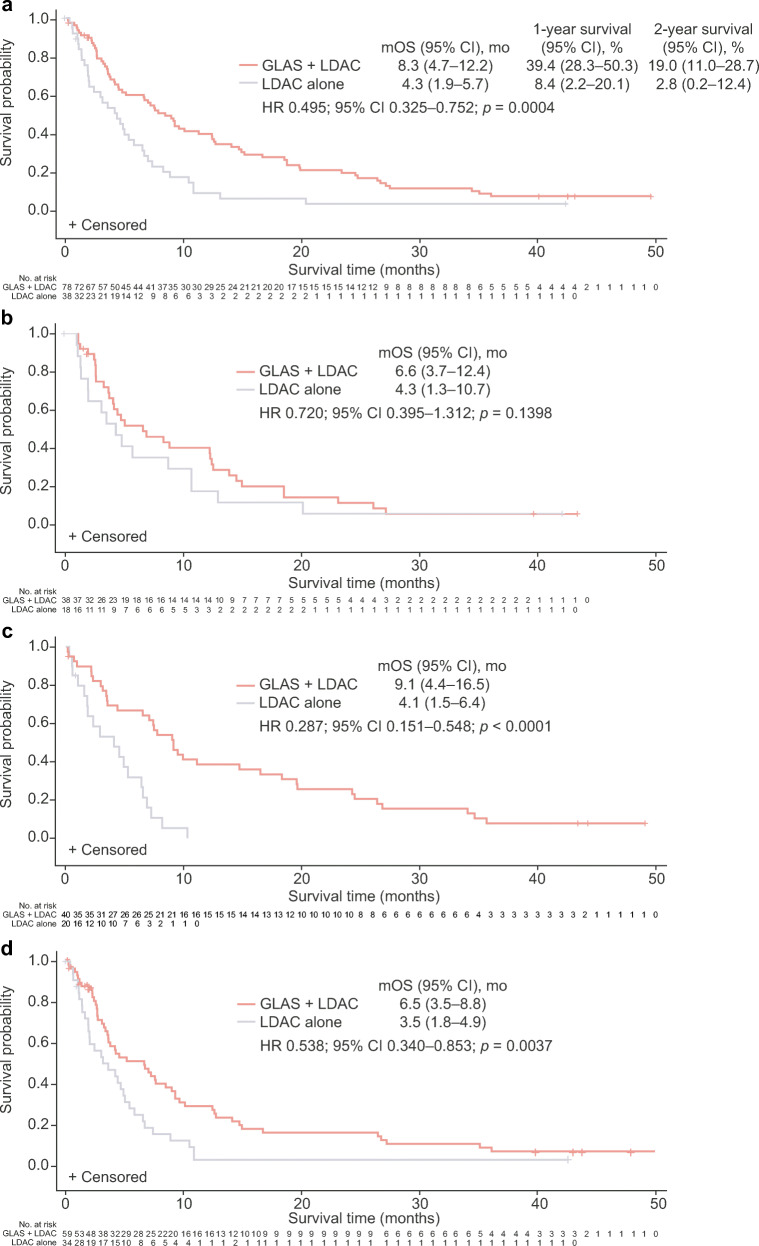
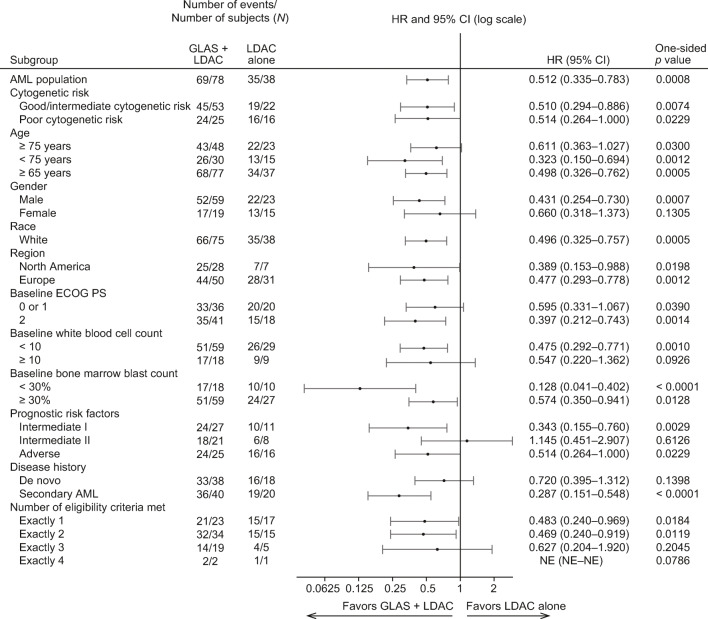
This analysis from the phase II BRIGHT AML 1003 trial reports the long-term efficacy and safety of glasdegib + low-dose cytarabine (LDAC) in patients with acute myeloid leukemia ineligible for intensive chemotherapy. The multicenter, open-label study randomized (2:1) patients to receive glasdegib + LDAC (de novo, n = 38; secondary acute myeloid leukemia, n = 40) or LDAC alone (de novo, n = 18; secondary acute myeloid leukemia, n = 20). At the time of analysis, 90% of patients had died, with the longest follow-up since randomization 36 months. The combination of glasdegib and LDAC conferred superior overall survival (OS) versus LDAC alone; hazard ratio (HR) 0.495; (95% confidence interval [CI] 0.325-0.752); p = 0.0004; median OS was 8.3 versus 4.3 months. Improvement in OS was consistent across cytogenetic risk groups. In a post-hoc subgroup analysis, a survival trend with glasdegib + LDAC was observed in patients with de novo acute myeloid leukemia (HR 0.720; 95% CI 0.395-1.312; p = 0.14; median OS 6.6 vs 4.3 months) and secondary acute myeloid leukemia (HR 0.287; 95% CI 0.151-0.548; p < 0.0001; median OS 9.1 vs 4.1 months). The incidence of adverse events in the glasdegib + LDAC arm decreased after 90 days' therapy: 83.7% versus 98.7% during the first 90 days. Glasdegib + LDAC versus LDAC alone continued to demonstrate superior OS in patients with acute myeloid leukemia; the clinical benefit with glasdegib + LDAC was particularly prominent in patients with secondary acute myeloid leukemia. ClinicalTrials.gov identifier: NCT01546038.
这项来自 II 期 BRIGHT AML 1003 试验的分析报告了不适合强化化疗的急性髓系白血病患者使用吉西他滨联合低剂量阿糖胞苷(LDAC)的长期疗效和安全性。这项多中心、开放标签研究将患者随机分为(2:1)接受吉西他滨联合 LDAC(初治,n=38;继发急性髓系白血病,n=40)或 LDAC 单药治疗(初治,n=18;继发急性髓系白血病,n=20)。在分析时,90%的患者已经死亡,自随机分组以来最长随访时间为 36 个月。与 LDAC 单药治疗相比,吉西他滨联合 LDAC 可显著改善总生存期(OS);风险比(HR)为 0.495;(95%置信区间[CI] 0.325-0.752);p=0.0004;中位 OS 为 8.3 个月与 4.3 个月。OS 改善在所有细胞遗传学风险组中均一致。在事后亚组分析中,在初治急性髓系白血病患者中观察到吉西他滨联合 LDAC 具有生存趋势(HR 0.720;95%CI 0.395-1.312;p=0.14;中位 OS 6.6 个月与 4.3 个月)和继发急性髓系白血病(HR 0.287;95%CI 0.151-0.548;p<0.0001;中位 OS 9.1 个月与 4.1 个月)。吉西他滨联合 LDAC 组在 90 天治疗后不良反应发生率下降:前 90 天内为 83.7%,而 90 天内为 98.7%。吉西他滨联合 LDAC 与 LDAC 单药治疗相比,在急性髓系白血病患者中继续表现出更好的 OS;吉西他滨联合 LDAC 的临床获益在继发急性髓系白血病患者中尤为显著。临床试验.gov 标识符:NCT01546038。