Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands
Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
J Nucl Med. 2021 Nov;62(11):1616-1623. doi: 10.2967/jnumed.120.255745. Epub 2021 Mar 19.
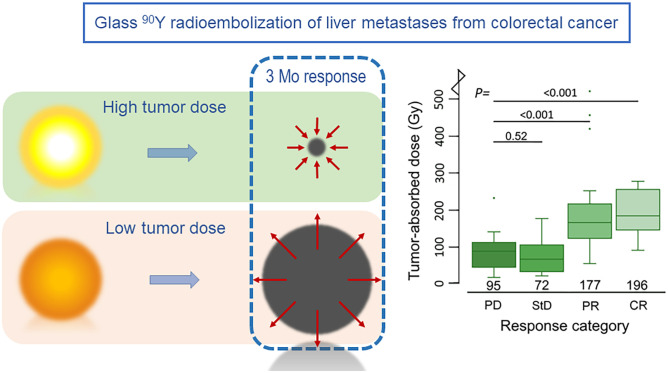
Radioembolization based on personalized treatment planning requires established dose-response and dose-toxicity relationships. The aim of this study was to investigate dose-response and dose-toxicity relationships in patients with colorectal liver metastases (CRLMs) treated with glass Y-microspheres. All CRLM patients treated with glass Y-microspheres in our institution were retrospectively analyzed. The tumor-absorbed dose was calculated for each measurable metastasis (i.e.,F-FDG-positive and more than a 5-cm tumor volume) on posttreatment Y PET. Metabolic tumor response was determined on F-FDG PET/CT by measuring the total lesion glycolysis at baseline and at 3 mo after treatment. The relationship between tumor-absorbed dose and metabolic response was determined on a per-lesion and per-patient basis using a linear mixed-effects regression model. Clinical toxicity and laboratory toxicity were correlated with healthy liver-absorbed dose. Thirty-one patients were included. The median tumor-absorbed dose of 85 measurable metastases was 133 Gy (range, 20-1001 Gy). Per response category, this was 196 Gy for complete response (CR), 177 Gy for partial response (PR), 72 Gy for stable disease, and 95 Gy for progressive disease (PD). A significant dose-response relationship was found on a tumor level, with a significantly higher tumor-absorbed dose in metastases with CR (+94%) and PR (+74%) than in metastases with PD ( < 0.001). A similar relationship was found on a patient level, with PR having a higher tumor-absorbed dose than did PD (+58%, = 0.044). A tumor-absorbed dose of more than 139 Gy predicted a 3-mo metabolic response with the greatest accuracy (89% specificity and 77% sensitivity), whereas a tumor-absorbed dose of more than 189 Gy predicted response with 97% specificity and 45% sensitivity. The median healthy liver-absorbed dose was 63 Gy (range, 24-113 Gy). Toxicity was limited mostly to grades 1 and 2, with 1 case of radioembolization-induced liver disease in a patient who received the highest healthy liver-absorbed dose. A positive trend was seen for most laboratory parameters in our dose-toxicity analysis. A significant relationship was observed between dose and response in CRLM patients treated with glass Y radioembolization.
基于个性化治疗计划的放射性栓塞需要建立剂量-反应和剂量-毒性关系。本研究的目的是研究玻璃 Y 微球治疗结直肠癌肝转移(CRLM)患者的剂量-反应和剂量-毒性关系。
我们机构中所有接受玻璃 Y 微球治疗的 CRLM 患者均进行了回顾性分析。在 Y 放射性核素治疗后 PET 上计算每个可测量转移灶(即 F-FDG 阳性且肿瘤体积大于 5cm)的肿瘤吸收剂量。通过测量基线和治疗后 3 个月时的总病变糖酵解,在 F-FDG PET/CT 上确定代谢性肿瘤反应。使用线性混合效应回归模型,基于病变和患者的基础,确定肿瘤吸收剂量与代谢反应之间的关系。临床毒性和实验室毒性与健康肝脏吸收剂量相关。
共纳入 31 例患者。85 个可测量转移灶的中位肿瘤吸收剂量为 133 Gy(范围,20-1001 Gy)。根据反应类别,完全缓解(CR)为 196 Gy,部分缓解(PR)为 177 Gy,疾病稳定(SD)为 72 Gy,疾病进展(PD)为 95 Gy。在肿瘤水平上发现了显著的剂量反应关系,CR(+94%)和 PR(+74%)转移灶的肿瘤吸收剂量明显高于 PD 转移灶(<0.001)。在患者水平上也发现了类似的关系,PR 的肿瘤吸收剂量高于 PD(+58%,=0.044)。肿瘤吸收剂量超过 139 Gy 可预测 3 个月的代谢反应,其准确性最高(特异性 89%,敏感性 77%),而肿瘤吸收剂量超过 189 Gy 可预测反应,特异性 97%,敏感性 45%。健康肝脏吸收剂量的中位数为 63 Gy(范围,24-113 Gy)。毒性主要局限于 1 级和 2 级,1 例患者因接受最高健康肝脏吸收剂量而发生放射性栓塞诱导的肝疾病。在我们的剂量-毒性分析中,大多数实验室参数都呈现出阳性趋势。
在接受玻璃 Y 放射性栓塞治疗的 CRLM 患者中,观察到剂量与反应之间存在显著关系。